



2Department of Thoracic Surgery, Bozyaka Training and Research Hospital, Izmir, Turkey
3Department of Pathology, Ege University School of Medicine, Izmir, Turkey
4Department of Obstetrics and Gynecology, Ataturk Training and Research Hospital, Izmir, Turkey DOI : 10.26663/cts.2018.00017
Summary
The incidence of coexistence of pregnancy and malignancy is approximately 1 in 1000-3000. Soft tissue sarcomas compose a very little portion of malignancies and Ewing’s sarcoma is one of these tumors, which is very rare, and the most lethal of all. We report a 37-year-old female at gestational age of 23 weeks with a rapidly growing tumor on the right chest wall and managed with chest wall resection and reconstruction. The togetherness of pregnancy and Ewing’s sarcoma is a rare entity and there is no exact information for treatment in the literature except a few case reports.Introduction
The incidence of coexistence of pregnancy and malignancy is approximately 1 in 1000-3000. Soft tissue sarcomas compose a very little portion of malignancies, and 137 cases were reported between the years of 1963-2016 and only 19 of these were Ewing’s sarcoma (ES) [1]. ES is one of these tumors, which is very rare, and the most lethal of all [2]. We present a case of ES underwent chest wall resection and reconstruction because of rapidly progressing mass on the chest wall by the onset of pregnancy.Case Presentation
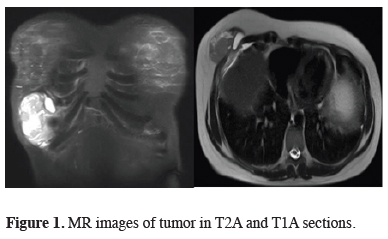
A 37 year-old female at a gestational age of 23 weeks (gravida: 2, para: 1) admitted with the complaints of pain and swelling on the right lower region of chest wall. Approximately a 6 cm diameter mass-like lesion was palpated on the lower region of right hemithorax. Laboratory findings were normal and β-hCG level was compliant with gestational age. A 70 x 35 mm diameter, heterogeneous mass with cystic components, elongating to intercostal area was detected in ultrasonography (USG). Magnetic resonance imaging (MRI) revealed a 75 x 44 mm mass invading sixth rib and causing irregularity on the contours of liver by compression with hyperintensity in T2A and iso-hypointensity in T1A sections (Figure 1). The patient was consulted with gynecology and obstetrics clinic, in consequence of obstetric USG showing compliant fetal findings with the gestational week, they mentioned the patient could be operated with close fetal monitoring.){kind=link}
 Click Here to Zoom |
Figure 1: MR images of tumor in T2A and T1A sections. |
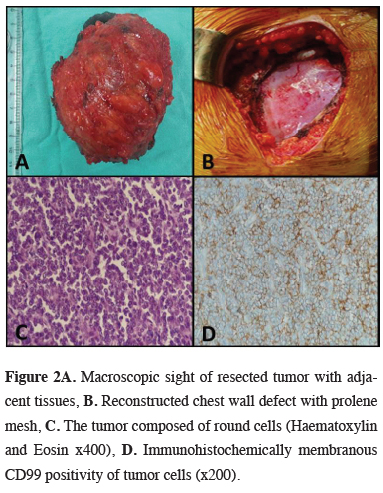
En-bloc resection of the mass with the invaded sixth rib and reconstruction by prolene mesh was performed. The postoperative course was uneventful. The patient was discharged on fourth day after the removal of thorax drain on third day. Histopathological examination reported an 8 cm diameter round cell sarcoma with bone invasion, immunohistochemical findings support Ewing’s sarcoma, resection margins were tumor-free (Figure 2).
){kind=link}
 Click Here to Zoom |
Figure 2A: Macroscopic sight of resected tumor with adjacent tissues, B. Reconstructed chest wall defect with prolene mesh, C. The tumor composed of round cells (Haematoxylin and Eosin x400), D. Immunohistochemically membranous CD99 positivity of tumor cells (x200). |
After histopathological diagnosis, the patient was followed up until the termination of pregnancy with a healthy newborn at the gestational age of 35 weeks. The oncologists planned adjuvant chemotherapy after evaluation with positron emission tomography. The patient is under follow up for nine months without any recurrence.
Discussion
Ewing’s sarcoma is a member of tumor family including peripheral primitive neuroectodermal tumors and Askin tumors [1]. Primary lesion is most commonly localized in femur, pelvic bones, humerus, fibula, clavicula or tibia, localization in rib, scapula and vertebrae is very rare. The rib localization has better prognosis. Initial findings are pain and tenderness by the growth of tumor [1,2].Multimodal therapies like chemotherapy, radiotherapy, surgery and combinations form the treatment of ES [3]. The main treatment include chemotherapy and surgical resection if possible. Treatment with radiation alone has declined in the past 30 years because of secondary malignancies due to radiotherapy, though it is a radio-sensitive tumor. The survival of patients whose primary tumor were resected is reported to be longer than the patients treated with chemo-radiotherapy [4].
Decision of mother and family is important for the type and time of the treatment. Chemotherapy can be planned according to the gestational age or it can be postponed after the termination of the pregnancy. In literature, successful treatment of ES by chemotherapy without any complication were reported but cases with fetal mortality secondary to chemotherapy were reported also [5]. The number of cases in literature is not enough for an exact decision for treatment. This is the first case, which underwent chest wall resection for ES during pregnancy. Surgical treatment was provided without any complication and gained time for chemotherapy, which might have serious side effects on fetus. Preoperative biopsy was not planned because of the tumor characteristics and to avoid tumor seeding if malignant. As a conclusion, resection should be offered for the treatment of ES in selected patients after the decision of family and other disciplines.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Reference
1) Zarkavelis G, Petrakis D, Fotopoulos G, Mitrou S, Pavlidis N. Bone and soft tissue sarcomas during pregnancy: A narrative review of the literature. J Adv Res 2016; 7: 581-7.
2) Verheecke M, Salembier C, Vanderlinden S. Delayed diagnosis of an Ewing sarcoma of the knee during pregnancy. Facts Views Vis Obgyn 2013; 5: 133-8.
3) Krasin MJ, Davidoff AM, Rodriguez-Galindo C, Billups CA, Fuller CE, Neel MD, et al. Definitive surgery and multiagent systemic therapy for patients with localized Ewing sarcoma family of tumors: local outcome and prognostic factors. Cancer 2005; 15; 104: 367-73.
4) Balamuth NJ, Womer RB. Ewing’s sarcoma. Lancet Oncol 2010; 11: 184-92.