



2Department of Thoracic Surgery, Medicalpark Antalya Hospital, Antalya, Turkey
3Department of Medical Oncology, Medstar Antalya Hospital, Antalya, Turkey
4Department of Nuclear Medicine, Medstar Antalya Hospital, Antalya, Turkey
5Department of Interventional, Medstar Antalya Hospital, Radiology Antalya, Turkey DOI : 10.26663/cts.2016.0006
Summary
Germ cell tumors arise from errors occurring during the migration of embryonic stem cells to the gonads. They constitute 10-15% of malignant mediastinal tumors. Thirty-nine years old male patient was admitted with shortness of breath and gynecomastia. Positron emission tomography / Computed tomography (PET/CT) showed hypermetabolic mediastinal mass in the anterior mediastinum. Serum tumor markers were elevated. Mixed germ cell tumor was diagnosed via transthoracic tru-cut biopsy. After three cycles of systemic cisplatin, etoposide and bleomycin treatment, PET/CT showed a decreased metabolic activity but an increase in the size of mass. "Growing teratoma syndrome" was diagnosed. The excision of the mass was performed via a median sternotomy. Then autologous stem cell transplantation was performed. Patients was presented as a successful example of a multimodality treatment of a primary mediastinal germ cell tumor with GTS.Introduction
Germ cell tumors are originated from the remnants of gonadal pluripotent cells during the embryological migration. Extragonadal germ cell tumors involve 75% of the mediastinal masses. More than 80% of mediastinal germ cell tumors are benign [1,2]. The "Growing teratoma syndrome" (GTS) is a rare condition which is seen in nonseminomatous germ cell tumors (NSGCT). Sometimes, the tumor growing is observed during or after a chemotherapy and named as GTS. It was first described in 1982 by Logothetis et al. and occurs in %2-7 of all NSGCT [3]. They defined three criteria which are, normalization of the serum tumor markers, an increase in the diameter of the mass and presence of mature teratoma in the resected specimen [3].In this case report we report the PET/CT findings a patient with GTS, and his successful treatment after a multidisciplinary planning.
Case Presentation
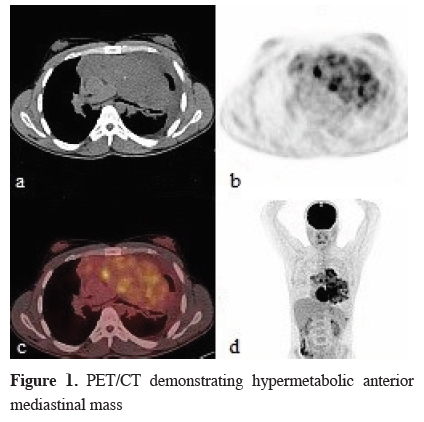
A thirty nine-years old male patient presented with bilateral gynecomastia and dyspnea for two months. On physical examination, decreased breath sounds on the left hemithorax, bilateral gynecomastia were observed. Genital examination was normal. Chest x-ray and thoracic computed tomography (CT) showed 17x8 cm mass covering the whole anterior mediastinum and pushing the heart to the right. The mass included micro calcifications and invaded vascular structures and pericardium. Positron emission tomography/Computed tomography (PET/CT) reported high metabolic activity in the heterogeneous mass lesion (SUVmax: 17.8) (Figure 1).){kind=link}
 Click Here to Zoom |
Figure 1: PET/CT demonstrating hypermetabolic anterior mediastinal mass |
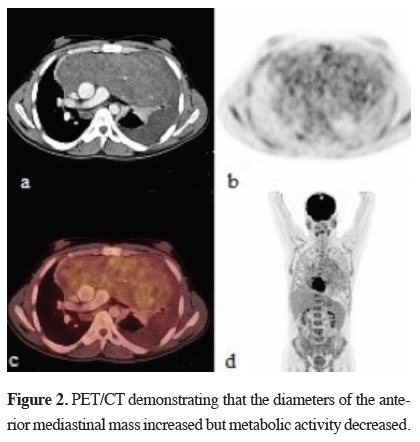
There was also a hypermetabolic nodule in the left pleural space and a non-metabolic left pleural effusion. Testicular ultrasound was normal. Serum AFP level was 3000 IU/dl (0-9 ng/mL), ß-hCG level was 555 IU/dl (0-2.67 mIU/mL). Pathologic diagnose was "mixed germ cell tumor" by CT guided tru-cut biopsy. The TNM classification was stage II. Three cycles of chemotherapy involving cisplatin, etoposide and bleomycin (BEP) therapy were applied. After the chemotherapy, patient was re-evaluated for treatment. PET/CT reported decreased metabolic activity (SUVmax: 5.5) but the tumor size increased to 21x9 cm (Figure 2).
){kind=link}
 Click Here to Zoom |
Figure 2: PET/CT demonstrating that the diameters of the anterior mediastinal mass increased but metabolic activity decreased. |
The AFP level was 14 ng/mL. The diagnosis of the overall examination was "Growing teratoma syndrome". Mediastinal mass was excised totally by median sternotomy. Macroscopic tumor size was 23 x 17 cm (Figure 3a). Pathological examination was reported as immature teratoma. Immature teratoma component originated from primitive mesoderm was 1-2%. Tumor included a necrotic area of %30-40 (Figure 3b).
){kind=link}
 Click Here to Zoom |
Figure 3: The pathologic findings of the resected tumor. a-The macroscopic view of mass, and b-histopathological view of immature teratoma (hematoxylin-eosin x 4). |
Post-operative AFP level decreased to 9.3 ng/mL and ß-hCG remained within normal limits. After high-dose chemotherapy contains isophosphomide, carboplatin and etoposide, autologous stem cell transplantation (ASCT) was performed. The patient has been in the remission for two years.
Discussion
Although mediastinal tumors are often asymptomatic, some symptoms such as chest pain, dyspnea, cough, and fever may occur. Symptoms are related the compression to vascular structures, airways and esophagus [1,2]. Teratomas can secrete hormones leading paraneoplastic syndromes as seen in this case.Determination of a mediastinal mass with radiological methods and elevation of serum AFP and ß-hCG may be enough for the diagnosis of NSGCT. Pathological examination provides an accurate diagnoses by revealing if an immature component exists. A tomography guided fine-needle biopsy or core biopsy can give a minimal invasive and successful diagnostic result. If this procedure is inadequate, it may be performed via a cervical mediastinoscopy, anterior mediastinotomy or thoracoscopy [4].
Mediastinal germ cell tumors frequently uptake FDG and PET/CT is used for staging and monitoring the metabolic response to chemotherapy, and also residue or recurrence of the tumor [5,6]. In this case the PET/CT was an essential tool for the diagnosis of GTS, showing a high metabolic activity and heterogeneity. After induction chemotherapy, the second PET/CT showed a decrease in the metabolic activity even though the diameters of the mass increased. The morphological and metabolic response mismatch findings supported the mixed nature of the mass [6].
The standard treatment of germ cell tumor must contain platinum-based regimen. The most common combination regimens are BEP (bleomycin etoposide, and cisplatin) and VIP (Isofosfamide, Etoposide, and Cisplatin) [7-9]. After three or four cycles of chemotherapy in case of full response, the patient must be followed without drugs. After chemotherapy, although tumor markers return to normal range, the mass grows up. In the presence of residual tumor or GTS surgical resection are proposed by most authors. [10-12] Sometimes the patient with GTS may refer in a bad condition and urgent operation may be necessary [10].
Sarkaria et al. [7] reported good prognostic factors in a series of 43% mixing type of totally 56 NSGCT patients as, R0 surgical resection after standard BEP chemotherapy, postoperative pathology demonstrates necrosis instead of teratoma, descending tumor marker levels after chemotherapy and prior stage I-II.
Walsh et al. [13] reported that an additional radical surgical resection to the initial standard or intensive chemotherapy after recurrence, increased the survey. Rodney et al. [14] suggested 3 poor prognostic factors as, serum ß-hCG level greater than 1,000 mIU/mL at diagnosis, presence of extra mediastinal disease and any mixed and single histologic diagnosis other than ectodermal sinus tumors. Accordingly in our case final pathological examination was reported as immature teratoma which is a prognostic factor.
Autologous stem cell transplantation following high-dose chemotherapy is defined as a treatment option for selected patients [8,15,16]. Bone marrow is affected by chemotherapy and regains the functions with ASCT. Bokemeyer et al [15] reported that according to "International Germ Cell Tumor Group Consensus Classification" the patients in the middle and poor prognosis groups benefit from high-dose chemotherapy and ASCT as a first treatment, instead of the standard treatment and the survey increases by %15. In this case, surgical excision followed by VIP chemotherapy and pathologic examination showed immature teratoma including 30%-40% necrosis. Although tumor markers and FDG uptake decreased the mass included more than 1% viable tumor cells so the high risk patient went to high-dose chemotherapy, and autologous ASCT.
In conclusion, we present this case as PET/CT findings of GTS was interesting, besides the patient was treated a successful instance of planning and treatment with medical oncology, thoracic surgery, hematology, and nuclear medicine clinics, i.e. multidisciplinary.
Declaration of conflicting interests
The author declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author received no financial support for the research and/or authorship of this article.
Reference
1) Hainsworth JD, Greco FA. Nonseminomatous malignant germ cell tumors of the mediastinum. In: Shields TW, Locicero J, Reed CE, Feins RH, editors. General Thoracic Surgery. Philadelphia: Wolters Kluwer Lippincott Williams&Wilkins; 2009. p. 2403-9.
2) Kang CH, Kim YT, Jheon SH, Sang S, Sung S, Kim JH. Surgical treatment of malignant mediastinal nonseminomatous germ cell tumor. Ann Thorac Surg 2008; 85:379-84.
3) Logothetis CJ, Samuels ML, Trindade A, Johnson DE. The growing teratoma syndrome. Cancer 1982; 50:1629-35.
4) Shinagare AB, Jagannathan JP, Ramaiya NH, Hall MN, Van den Abbeele AD. Adult extra gonadal germ cell tumors. Am J Roentgen 2010; 195: 274-80.
5) Rankin S. 18F-2-Fluoro-2-deoxy-d-glucose PET/CT in mediastinal masses. Cancer Imaging. 2010; 10(1A): S156-S160.
6) Agatsuma T, Koizumi T, Kubo K, Saito G, Kondo R, Yoshida K, et al. Mediastinal growing teratoma syndrome successfully treated by multiple modality therapies. Intern Med 2011; 50: 607-10.
7) Sarkaria IS, Bains MS, Sood S, Sima CS, Reuter VE, Flores RM, et al. Resection of primary mediastinal non-seminamatous germ cell tumors: A 28-years" experience at Memorial Sloan-Kettering Cancer Center. J Thorac Oncol 2011; 6: 1236-41.
8) Date H, Kiura K, Ueoka H, Tabata M, Hotta K, Katayama H, et al. Induction chemotherapy, surgical resection, and high-dose chemotherapy for mediastinal nonseminamatous germ-cell tumor. J Thorac Cardiovasc Surg 2003; 130: 1205-6.
9) Iyoda A, Hiroshima K, Yusa T, Toyozaki T, Fujisawa T, Ohwada H. The primary mediastinal growing teratoma syndrome. Anticancer Res 2000: 20(5C): 3723-6.
10) Kesler KA, Patel JB, Kruter LE, Birdas TJ, Rieger KM, Okeroke IC, et al. The "growing teratoma syndrome" in primary mediastinal nonseminomatous germ cell tumors: Criteria based on current Practice. J Thorac Cardiovasc Surg 2012; 144: 438-43.
11) Li-Tzong Chen, Cheng-Lung Chen, and Wei-Shou Hwang. The growing teratoma syndrome. A case of primary mediastinal nonseminomatous germ cell tumor treated with chemotherapy and Radiotherapy. Chest 1990; 98: 231-3.
12) Tongaonkar HB, Desmane VH, Dalal AV, Kulkarni JN, Kamat MR. Growing teratoma syndrome. J Surg Oncol 1994; 55: 56-60.
13) Walsh GL, Taylor GD, Nesbitt JC, Amato RJ. Intensive chemotherapy and radical resections for primary nonseminomatous mediastinal germ cell tumors. Ann Thorac Surg 2000; 69: 337-44.
14) Rodney AJ, Tannir NM, Siefker-Radtke AO, Liu P, Walsh GL, Millikan RE, et al. Survival outcomes for men with mediastinal germ-cell tumors: The university of Texas M.D Anderson Cancer Center experience. Urol Oncol 2012; 30: 879-85.