



2Department of Thoracic Surgery, Yildirim Beyazit University, Yenimahalle Education and Research Hospital, Ankara, Turkey
3Department of Thoracic Surgery, Adiyaman University Education and Research Hospital, Adiyaman, Turkey
4Department of Thoracic Surgery, Yildirim Beyazit University, Faculty of Medicine, Ankara, Turkey DOI : 10.26663/cts.2019.00027
Summary
Bronchogenic cysts are generally asymptomatic and are detected incidentally by radiographic imaging as a smooth homogeneous mediastinal/pulmonary lesion. Isolated intradiaphragmatic bronchogenic cysts are extremely rare. Here, we report a case of intradiaphragmatic bronchogenic cyst mimicking a left lower lobe mass in a 56-year-old man suffering from chest pain. Imaging studies of the chest, including plain chest radiography and computerized tomography revealed a left sided mass in the lower zone. The patient underwent surgical resection of the mass. Intradiaphragmatic bronchogenic cyst was diagnosed by pathology.Introduction
Bronchogenic cysts are uncommon congenital anomalies of foregut origin. They are most frequently found in tracheobronchial tree, mediastinum or within the lung parenchyma. Rarely, the cysts have occurred in other locations. They are generally asymptomatic in the adulthood age. They can cause symptoms only when infected, ruptured or pressing on neighbouring structures. Most of them presented as a smooth homogeneous water density shadows mediastinal or pulmonary opacity on chest radiographs or computed tomography (CT). If the cysts are asymptomatic or diagnosed in any way, to avoid possible complications should be treated by surgery [1,2].Case Presentation
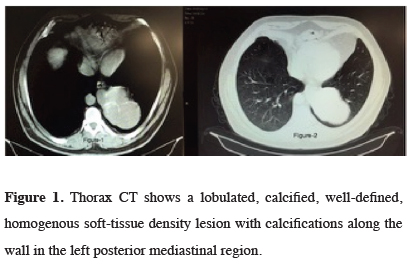
Our patient, a 56-year-old man, was referred to our institution for chest pain of one year duration. General physical examination and routine laboratory tests were unremarkable. The thorax CT revealed a lobulated, calcified, well-defined, and homogeneous mass, of 6x8x6 cm at the lower zone (Figure 1).){kind=link}
 Click Here to Zoom |
Figure 1: Thorax CT shows a lobulated, calcified, well-defined, homogenous soft-tissue density lesion with calcifications along the wall in the left posterior mediastinal region. |
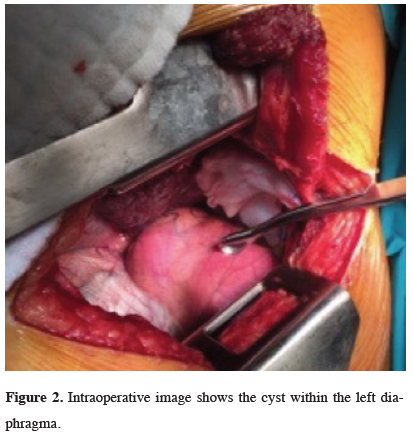
A left thoracotomy was performed for the resection of the lesion. Intraoperatively, a 6x8 cm sized cyst was found within the left hemidiaphragma. The mass has no connection with the left lung parenchyma. It was enucleated from the left hemidiaphragma (Figures 2,3). The diaphragma was repaired with a 6x8 cm sized polypropylene mesh. There were no intraoperative complications.
){kind=link}
){kind=link}
 Click Here to Zoom |
Figure 2: Intraoperative image shows the cyst within the left diaphragma. |
 Click Here to Zoom |
Figure 3: Excised cystic lesion. |
On gross examination, the cystic mass was multilocular, thin-walled and filled with red, yellow fluid. On microscopic sections, the cyst had smooth muscle tissue, cartilage and mucus glands on its wall. It was lined with ciliated cylindrical respiratory mucus epithelium, thus established a histopathologic diagnosis of intradiaphragmatic bronchogenic cyst.
Discussion
Bronchogenic cysts are uncommon congenital anomalies of foregut origin [1]. They are most frequently found in tracheobronchial tree, mediastinum. Extra mediastinal bronchogenic cysts may be located in the lung parenchyma, diaphragma or pleura [2]. Intrapulmonary cysts are usually found in the perihilar areas or rarely peripherally in the lower lobe. In our case, the cyst was found in diaphragma but on CT plains it appears as located in lower lobe.Bronchogenic cyst is the most common mass lesion in diaphragma in general population and the most common benign cystic process in infants. They are observed within congenital cysts [3,4]. Two-thirds of the patients are asymptomatic and the cyst is detected incidentally. Symptomatic patients generally present with chest pain, cough, dyspnea, fever and dysphagia. Chest pain is the most frequent symptom. In our case, chest pain complaint was observed as symptom and lesion was detected during radiographic examination.
It is often enough to apply plain chest radiography, thorax CT and bronchoscopy from among the laboratory methods for diagnosis. On plain film examinations, bronchogenic cysts present as spherical or oval masses with smooth outlines and soft tissue. CT is an excellent method for demonstrating the size, shape, position and margin characteristics of the cyst. It is also useful to show mass effect on adjacent structures, cyst attenuation, homogeneity and calcification. Barium swallow can be useful in dysphagic cases. In our case, radiology, especially CT, helped to a great extent about lesion’s nature, placement and size.
Life-threating complications such as airway obstruction, atelectasis, and compression are reported in pediatric age group. It is reported in current series that bronchogenic cysts in adults are more symptomatic. In our case, though it is adult, complications such as respiratory distress related with compression, atelectasis, and infection were not reported.
The cyst may show a solid appearance because of infection and its density increasing in parallel with its protein/calcium content. Cyst hydatid, lung abscess, infected air cyst, cavitary disease and malignancy should be kept in mind in differential diagnosis [2,5]. Bronchogenic cysts containing mucoid material are surrounded by a wall of bronchial cartilage, smooth muscle, elastic tissue and mucous gland [6,7]. In our case similar histopathological findings were reported.
Surgery may be considered as a treatment of choice even if the cyst is asymptomatic, to avoid complications such as infection, haemorrhage, or neoplasia within the cyst. Observation may be indicated for small, classic, asymptomatic cysts or high-risk patients.
Percutaneous catheter, drainage, sterile alcohol ablation or transbronchial cyst aspiration have been performed in selected cases [8,9]. Total excision of mediastinal bronchogenic cysts is adequate for treatment, minimal (wedge), segmental or lobar resection may be needed in parenchymal bronchogenic cysts [10].
Consequently, bronchogenic cysts must be kept in mind in all cystic lesions, in suppurated cyst appearance or in cases when tumor is not marginalized.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Reference
1) Shami FM, Sachs HJ, Perkins DG. Cystic disease of the lungs. Surg Clin North Am 1988; 68: 581-620.
2) Armstrong P, Padley S. The Mediastinum In: R G.Grainger, D J Allison, A. Adam, A K. Dixon, eds.Grainger and Allison’s diagnostic radiology, fourth edition, volume 2, London ; Churchill Livingstone 2001: 364-5.
3) Anderson LS, Forrrest JV. Tumors of the diaphragm. Am J Roentgenol 1973; 119: 259-65.
4) Olafsson G, Rousing A, Holen O. Primary tumors of the diaphragm. Chest 1971; 59: 568-705.
5) Okur E, Altan K, Okur H, Ertuğrul M, Halezaroğlu S, Atasalihi A. Bronkojenik kistlerde cerrahi tedavi. Toraks Dergisi 2002; 3: 66-9.
6) Ribet ME, Copin MC, Gosselin B. Bronchogenic cysts of the mediastinum. J Thorac Cardiovasc Surg 1995; 109: 1003-10.
7) Battistella FD, Benfield JR. Blunt and penetrating injuries of the chest wall, plevra and lungs. In: Shields TW, Lo Cicero J, Ponn RB, editors. General thoracic surgery. 5th ed. Philadelphia: Lippincott Williams & Wilkins, 2000. p. 815-832.
8) McAdams HP, Kirejczyk WM, Rosado-de-Christenson ML, Matsumoto S. Bronchogenic cyst: Imaging Features with Clinical and Histopathologic Correlation. Radiology 2000; 217: 441-6.