



2Institute of Biomedical Engineering, Bogazici University, Istanbul, Turkey DOI : 10.26663/cts.2020.00012
Summary
Background: The present invention relates to a medical device that enables the “automatic” bending of the pectus bar. The curved bar is used in the correction of the deformities of the sunken chest (pectus excavatum) and the pigeon’s chest (pectus carinatum).Materials and Methods: Conventionally, the surgeon shapes pectus bars manually during the surgery by trial/error method. In these surgeries, it may not be possible to give the ideal shape manually each time due to the complex anatomy of the patients’ deformity, which might lead to increases in the operation time and the risk of complications (organ injury, bleeding, etc.). The present invention aims to prepare a customized preoperative bent bar by using the CT coordinates of the deformity by the surgeon via a custom software. Besides, as an alternative method, as usual, the novel automated bender can copy a soft metal template.
Results: We presented this project to a few national and international companies. A national company has decided to take the project seriously about starting the process of producing the automatic bender to be used in the related field. The patent has protection both nationally and internationally.
Conclusions: This patent will probably change the clinical pectus bar bending process providing excellent results with high satisfaction rates for both the patients and the surgeons.
Introduction
The Nuss procedure is now the preferred operation for the surgical correction of pectus excavatum (PE) [1]. It is a minimally invasive technique, whereby up to three curved metal bars are inserted behind the sternum to push it into a normal position. The bars are left in situ for three years and then removed. This procedure significantly improves the quality of life and, in most cases improves cardiac performance.Pectus excavatum is the most common anomaly of the anterior chest wall. Correction of the PE significantly increases the quality of life for the patients and, in most cases improves their cardiac performance [2,3]. Since Ravitch published his first paper in 1949, a modified Ravitch approach with resection of cartilage has been the preferred operation for surgical correction of PE in most surgical units [4]. After Nuss published his minimally invasive Nuss procedure in 1998, whereby curved bars are inserted behind the sternum to position it anteriorly, it has changed the treatment of PE and become the most commonly used technique [5]. It results in improved cosmesis regarding both the shape of the anterior chest wall and the absence of an incision anterior to the sternum.
The original technique, the bar bending, is being performed “manually” using a soft metal template that gets the shape of the patients’ chest wall deformity. This novel invention facilitates and improves the accuracy of the bar bending process. The bender copies the soft metal template as in the classical method. Besides, it uses the digital coordinates of the chest wall deformity acquired through the custom software that extracts the coordinates of the chest wall deformity from 3D-CT images. The bender uses the coordinates to bend the pectus bar that is placed into the automatic bender preoperatively (pre-bent bar). The bender can also curve the bar during the surgery as needed to get optimal results in shorter surgery time.
In this manuscript, we described this novel pectus bar bending system in detail.
Methods
Surgeons bend the pectus bars manually in the present setting. The surgeon determines the final form of the patient’s deformity using a soft metal template while the patient is lying in the supine position. Then, using the bending tools on the back table, the surgeon tries to give the shape of the soft metal template to the original metal bar to be used for the patient. This is not always the case, especially in complicated asymmetric deformities and in the hands of inexperienced surgeons.The present invention makes this process more precise, more accessible, and automated. The physicians will have two options for the bending process. First, they can use the soft metal template (conventional method) and second preoperative 3D-CT (thorax) coordinates of the deformity to bend the pectus bar accordingly. The surgeon can use the cursor on the monitor to determine the shape, length, and entry and exit points of the metal bar. The desired optimal shape to the original pectus bar can be generated before and during the surgery as well.
The provisional patent application (TKNK/030059/000060) (Specification: 30.10.2017) is completed in collaboration with Boğaziçi University, Institute of Biomedical Engineering. The patent owner is now the Boğaziçi University. We have prepared a clinical trial project related to the novel bar bender. It was necessary to prepare the ethics committee document from the front. We had to clarify the financial resources for the study. We applied for support to our project to The Scientific and Technological Research Council of Turkey. However, due to not being in University staff, our application is rejected. Upon searching for financial assistance, we came across the Small and Medium Enterprises Development Organization of Turkey (KOSGEB) supports. The new plan is to transfer the patent right of use to a biotechnical company located in Ankara to apply for the KOSGEB support and produce our product to be used in the clinical setting.
After producing the automated bender machine, the plan is to bring it to the clinics who needs and who are allocated in the clinical trial free in the first year. Besides, we will provide the pre-bent bars to the clinics which request remotely (bar cost will be charged). After the first year, we will charge an affordable price for both the whole bender machine and the pre-bending process.
Results
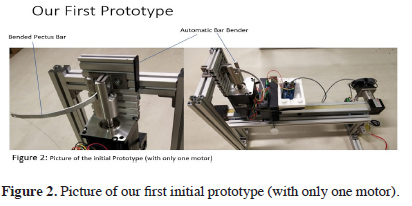
The “Automatic Bar Bender” is seen in Figures 1 ac and Figure 2. Besides, the initial prototype is watched at the Video -1 and Video -2 and the photo.
Video-1. The initial prototype of “Automatic Bar Bender” (real),
Video-2. Animated application for bar bending.
 Click Here to Zoom |
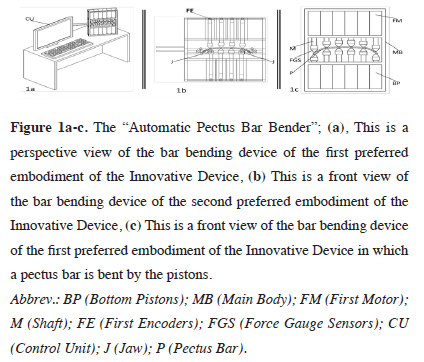
Figure 1a-c: The “Automatic Pectus Bar Bender”. |
 Click Here to Zoom |
Figure 2: Picture of our first initial prototype (with only one motor). |
In the present invention, a soft metal-based guide strip bar, which is pre-shaped manually by placing directly on the skin of the patient’s deformity (as in the current clinical setting), could be copied by the automatic bender machine using a key-copying method. There is no need to use manual benders easing the bar shaping process for all surgeons in the field.
Besides, the new bender machine could get the 3D-CT coordinates of each patients’ deformity to process. The encoder, which has the geometry of the deformity, is then inserted into the two rows of pistons of the automatic pectus bar-bending device and advanced from the initial position until each piston contacts the guide bar. The length of the piston shaft at the point where the force sensors contact the guide is connected to each piston separately. The automatic bender takes into account the 3D-CT coordinates during the whole bending process to get an optimal result for shaping the pectus bar.
Thanks to the control unit, the relevant coordinates are recorded. In this way, the deformity geometry of the patient can be transferred to the digital environment in a much cheaper and practical way without the need for expensive medical imaging methods. Then the shape that the pectus bar should take to correct this deformity is created by the software of the device and finalized by the surgeon. The final bar geometry is applied to the pectus bar, which is initially placed flat within the bar shaping device.
Detailed Description of the Innovative Device
A preferred embodiment of the Innovative Device is shown in (Figures 1 ac). In this form, the hydraulic or pneumatic base pistons (BP), which can move independently of each other, are placed in the main body (MB) in the form of two rows in a single plane. To move the pistons, initial motors (FM: preferably servo-motor) connected to each piston shafts (M) and controlled in a forward/reverse motion, and encoders (FE) connected to these initial motors. Sensors (FGS; e.g., force gauge sensors) are disposed at the second facing ends of the oppositely disposed pistons (BP). The data from these FGS and the data received from the initial encoders (FE) are recorded, processed by a control unit, and the necessary electrical signals controlling the first motors (FM) are generated and transmitted to the said initial motors (FM).
){kind=link}
The control unit of automatic bar bender comprises a processor, memory unit, data input interface (e.g., keyboard, mouse, touch screen, etc.), a data input connector that provides a data connection between the main body (MB) and or Bluetooth, Wi-Fi and so on. An electronic device comprising a wireless data communication module such as a desktop computer, laptop computer, tablet computer, and the like can be any electronic device. Besides, this control unit comprises a graphical user interface for communicating with the user and a display device like a monitor, touch screen, etc., for displaying this graphical user interface to the user.
In the second embodiment of the Innovative Device, at least one-third motor including at least one-third encoder (rotational encoder) which can be rotated about the central axis, which can be moved independently of one another, besides the hydraulic or pneumatic bottom pistons (BP) positioned perpendicular to the pectus bar (P) and at least one jaw (J) rotated by said at least one-third motor (preferably servo motor).
In this embodiment of the present Innovative Device, this control unit (CU) comprises of a desktop computer, laptop computer with a data input connector (or a wireless data communication module such as Bluetooth, Wi-Fi, etc.) that provides a data connection between the processor, memory unit, a data input interface (e.g., keyboard, mouse, etc.), MB, tablet computer, etc., can be any device. Besides, this CU comprises a display device with a graphical user interface for communicating with the user and a monitor, touch screen, etc., for displaying this graphical user interface to the user.
As described technically above, the idea is to bend the pectus bar automatically either by key copying method using the standard bent soft metal template and the 3D-CT image coordinates of the chest wall deformity for creating an ideal bent pectus bar customized for each patient.
Discussion
The Ravitch procedure was developed for the surgical treatment of congenital chest wall deformities, including pectus excavatum and pectus carinatum. These congenital abnormalities are thought to result from an abnormal overgrowth of the rib cartilage adjacent to the sternum, displacing the sternum anteriorly, resulting in pectus carinatum; posteriorly, resulting in pectus excavatum; or both anteriorly and posteriorly, resulting in an asymmetric deformity [6].Pectus excavatum may be noted at birth and may become more pronounced when the child experiences rapid skeletal growth during adolescence. The exact mechanism underlying abnormal cartilage growth in pectus deformities is unknown.
Ravitch proposed the first technique of pectus excavatum repair in 1949, an open method that required partial resection of the cartilage, xiphoid excision, and osteotomy of the sternum [4]. Since then, surgical procedures have evolved towards more minimally invasive techniques. The introduction of the Nuss procedure (1998) was a radical paradigm shift [7].
The Nuss procedure is a minimally invasive alternative to the Ravitch procedure for the treatment of pectus deformities. It involves only internal bracing without resection of the abnormal cartilage [8]. It aims to force the sternum forward and hold it there with an implanted steel bar, but without performing a long incision to resect the abnormal cartilage [5]. In this procedure, the curved steel bar is placed under the sternum through two small incisions on the sides of the chest wall. Because the sternum is forced outward and held under high-pressure, the Nuss procedure results in more pain and discomfort than the modified Ravitch procedure. The steel struts must remain in place for approximately 2-4 years to properly reform the chest.
While less invasive than the Ravitch procedure, the initial Nuss procedure surgery still requires 4-5 days of hospitalization for pain management due to the rather drastic change in chest shape [9]. Full recovery can take several weeks, during which time the patient’s physical activities are restricted. For both the modified Ravitch and the Nuss procedures, the bar removal operation is a much simpler outpatient surgery, and the patient can usually leave within a couple of hours.
In conventional surgical corrections for pectus deformity, one or two metal bars (Lorenz Bars) are selected according to the patient, the depth and extent of the deformity. These pectus bars are placed under the sternum under general anesthesia with video-assisted thoracoscopic surgery (VATS). The Lorenz bar is brought to its final shape manually during the operation by using shaping, curving, and corrective hand tools on the back-table. This process can take 25-30 minutes in the competent hands, but in the inexperienced hands, it can take longer than one hour. It may need to be repeated several times during the surgery, which might increase the surgical complications such as organ injury, bleeding, prolonging of the procedure and the anesthesia time, etc.
To our knowledge, there is no automatic bender/molder in the literature using both the copying of the standard soft metal template and also the 3D- CT image coordinates of the chest wall deformities to bend the original pectus bar pre and intraoperatively.
In summary, the prostheses (pectus bars) used in pectus excavatum and carinatum deformities are shaped by the surgeon during the surgery by trial/error method, as mentioned above. In these surgeries, it may not be possible to give the ideal shape each time, depending on the complex asymmetric anatomy of the patient’s deformity during the bending of the bar specific to the patient by using bending hand tools.
Besides, since the desired geometry can be achieved at one time during this process, which requires physical strength and experience, it is often necessary to repeat this process several times during the insertion process of the bar. In other words, after placing the pectus bar under the sternum at the required level, it is most of the time necessary to remove it again outside the body when some final corrections and re-insertion processes are needed. Re-insertion sessions lead to an increased risk of complications (organ injury, bleeding, etc.) as well as prolonging the surgery time and late complications as prolonged pain, displacement of the bar, and even fracture of the bar.
This new patent-pending apparatus would ease and shorten the bending process of the pectus bar and increase the possibility of optimally bending a customized bar for each patient. The unique bending process could decrease the complications rates, the time for surgery and hospital stay, and on the contrary, increase the success rates and the patients’ satisfaction rates.
In conclusion, the benefits for such ‘an automatic bar bender’ are providing a customized optimal bar shape for each patient, which decreases the complication rates and the time for the surgery, anesthesia, and hospital stay.
Additionally, such a process could ease the optimal bar bending process helping all thoracic surgeons who wish to perform the non-invasive pectus surgery with a high success rate.
Lastly, after the analyses of the 3D-CT coordinates using the specific software, a report including suggestions for the optimal bar insertion and exit points, optimal bar length, and bar numbers to be used, the Haller Index and the volume of the sunken deformity could be given to the surgeon.
To sum up, all described points related to such a new automatic bar bender could change the game played in the field of pectus surgery.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received financial support from Small and Medium Enterprises Development Organization of Turkey (KOSGEB) for the research.
Reference
1) Pilegaard HK. Short Nuss bar procedure. Ann Cardiothorac Surg 2016;5:513-518.
2) Maagaard M, Tang M, Ringgaard S, Nielsen HH, Frøkiær J, Haubuf M et al. Normalized cardiopulmonary exercise function in patients with pectus excavatum three years after the operation. Ann Thorac Surg 2013;96:272-8.
3) Udholm S, Maagaard M, Pilegaard H, Hjortdal V. Cardiac function in adults following minimally invasive repair of pectus excavatum. Interact Cardiovasc Thorac Surg 2016;22:525-9.
4) Ravitch MM. The operative treatment of pectus excavatum. Ann Surg 1949;129:429-44.
5) Nuss D, Kelly RE Jr, Croitoru DP, Katz ME. A 10-year review of a minimally invasive technique for the correction of pectus excavatum. J Pediatr Surg 1998;33:545-52.
6) Abdullah F, Harris J. Pectus excavatum: more than a matter of aesthetics. Pediatr Ann 2016;45:e403-e406.
7) Nuss D. Recent experiences with minimally invasive pectus excavatum repair “Nuss procedure”. Jpn J Thorac Cardiovasc Surg (Internet) 2005;53:338-44.