



2Department of Thoracic Surgery, Gulhane Training and Research Hospital, Ankara, Turkey DOI : 10.26663/cts.2018.0008
Summary
Background: Rib fractures occur usually after thoracic traumas. Multiple and displaced fractures are occasionally associated with respiratory complications. That is why treatment for rib fractures should be done properly to prevent respiratory complications. This experimental study was performed to investigate the effects of early and late period rib fixation, on respiratory functions in an animal model with multiple displaced rib fractures, and to design a multiple displaced rib fracture treatment model.Materials and Methods: Twenty-four, New Zealand rabbits were used in this study. The subjects are divided into three groups. All subjects’ three consecutive ribs on right hemithorax were fractured and displaced surgically. Subjects in group I were observed without any further surgical process. In group II, subjects were undergone to a second surgery process to fix the fractured two ribs by titanium plate one week after the initial operation. In group III, subjects’ three consecutive ribs were fractured and two ribs were fixed by titanium plates at the same operation session. Then subjects’ respiratory functions, survivals and health status were observed.
Results: Oxygen saturation in first week (p = 0.032), clinical survival and health status were better than the other groups in group III. Fracture healing was better in fixation groups, radiologically and clinically.
Conclusions: Early rib fixation operation is recommended for multiple displaced rib fractures to prevent secondary respiratory complications.
Introduction
Trauma is the major cause of deaths in the first four decades [1]. 20-25% of traumatic deaths are due to thoracic trauma and 25-50% of the remaining are accompanied by thoracic trauma [2,3]. About 60% of the patients with multitrauma have thoracic trauma, with 30-40% of them having rib fractures [4-6]. As it is so frequent, it should be treated appropriately.The major goal in the treatment of patients with rib fractures is providing analgesia. If pain control is not optimized, complications such as atelectasis and infections are more frequently encountered [1-7]. It has been reported that, treatment options in patients with multiple rib fractures are associated with the number of fractures, location, age of the patient, and lung status [8-10]. Common indications for surgical treatment of rib fractures are flail chest, chest wall deformities / defects, pain, nonunion of fractures, symptomatic patients with three or more consecutive rib fractures [10-13].
On the other hand, surgical treatment of rib fractures is still controversial. There are numerous publications showing that early stage fixation (stabilization) is effective in preventing significant morbidities such as pain and infection in addition to a positive effect on lung function. Our clinical experience supports these findings, but there are no controlled animal experiments about this controversy. The aim of our study is to investigate effects of rib fixation surgery on respiratory functions in an experimental animal model.
Methods
Gulhane Military Medical Academy Animal Experiments Ethics Committee approved the study (12/2013-13/134). 24 New Zealand rabbits were used in the study. All subjects were adult females with an average weight of 3378 ± 405 gr. Subjects were subjected to humanitarian treatment in accordance with the Laboratory Animals Care and Use Guide. The number of subjects was determined by statistical preliminary study. The subjects were divided into 3 groups with equal numbers. There was no food or fluid restriction on subjects on preoperative period.
Surgery
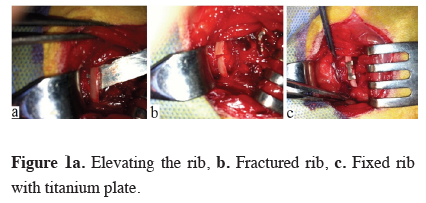
After anesthesia and endotracheal intubation, the skin and subcutaneous layers were opened while the subject was in the right side up position followed by opening the periosteum of the ribs (Figure 1a). In group I (n=8) three consecutive ribs of the subjects were surgically fractured and displaced. The subjects were observed without rib fixation surgery (Figure 1b).
In group II (n=8) three consecutive ribs of the subjects were surgically fractured and displaced. After seven days as a late fixation model, subjects were performed rib fixation surgery on two displaced ribs with titanium plaques (Figure 1c). In group III (n=8) three consecutive ribs of the subjects were surgically fractured and displaced. As an early fixation model, subjects were performed rib fixation surgery on two displaced ribs with titanium plaques, concurrently.
){kind=link}
 Click Here to Zoom |
Figure 1a: Elevating the rib, b. Fractured rib, c. Fixed rib with titanium plate. |
After surgery, medical treatment; antibiotherapy (Penicillin G 50.000 U/kg) and analgesic (Flunixinmeglumin 1.1 mg/kg) were ordered to the subjects for 3 days.
The subjects were taken into the cages alone at the postoperative period. All groups were followed in terms of their weight, heart and respiratory rate, chest x-ray, complete blood count (CBC) and, arterial blood gas sampling (ABG). During the follow-up period, attention was paid for adequate food and fluid intake, appropriate ambient temperature, being away from stressor factors (intense noise, light etc.) and giving appropriate medical treatment. Daily activity levels, food and water interest and, resting postures (pain posture) were observed. The effects of fixation on respiratory functions and healing process were evaluated in the obtained data. The animals were sacrificed on 3rd week under general anesthesia.
Statistical Analysis The relationship between survival time, pre and postoperative weights, respiratory and pulse rates, saturation values, ABG and CBC parameters of the experimental groups were determined in the SPSS 15.0 package program; as well as the descriptive analyzes; Kaplan-Meier, Chi-Square and Anova tests were used. A 3-week survival analysis was performed assuming that all subjects lived at least 1 day. The results were considered statistically significant when p < 0.05.
Results
A total of 24 operations were applied in 3 groups. In groups I,II and III, the number of subjects lost during surgery were 2,3 and 1 respectively (Table 1).){kind=link}
Table 1: Life span of subjects.
Although the average weights of subjects generally decreased, there was no significant difference between the groups at the end of the study (p = 0.280). Respiratory and pulse rates were compared, there was no significant difference between the preoperative and postoperative periods (p = 0.870 and p = 0.514 respectively). The oxygen saturation values were found better in early rib fixation group (group III) than the other two groups in first week and the difference was statistically significant (p = 0.032) (Table 2).
){kind=link}
Table 2: Mean saturation levels of groups at the postopera-tive first week.
During daily follow-up, subjects in the group III were found to be more active at the early postoperative period. Daily activity, food/water interest and pain posture were better in the group III than the other two groups.
Healing of fractured ribs was followed by chest x-ray. In group I, at the third postoperative week, it was observed that fractures were not healed and there was a significant fracture line. At postoperative 7th week there was a minimal fracture healing with callus. In group III, the fixed ribs were found to heal properly without significant callus tissue in the chest x-ray even at the postoperative first week. Also it is seen that unfixed ribs healed with significant callus tissue (Figures 2a,2b).
){kind=link}
 Click Here to Zoom |
Figure 2a: Fixed and unfixed ribs in x-ray, b. Significant callus tissue in chest x-ray. |
In the third group (early fixation model), the estimated life expectancy was 14.6 days; in the group II (late fixation model) the estimated life expectancy was 8.6 days; the estimated mean life span in the first group was 8.5 days.
There was no statistically significant difference between the two groups when compared with the groups Chi-square test (p = 0.750, p = 0.224, p = 0.402 respectively). However, it was accepted that the third group was clinically significant because the average life span was higher than the other groups (Table 3).
){kind=link}
Table 3: Mean survival of groups in Kaplan-Meier analysis.
The subjects were followed up for daily food and water consumption. The average weight of the first group before surgery was 3230 g; second group 3133 g; the third group was identified as 3770 g. In general, all groups were found to have weight loss. At the end of the study, the average weight of the subjects in the first group was 2830 g; the average weight of the subjects in the second group was 2965 g; the average weight of the subjects in the third group was 3414 g. Weight losses calculated as grams per day and percentages, differences compared with Kruskal-Wallis test. There was no significant statistical difference between the groups (p = 0.280).
The mean saturation value of the subjects in the first group before surgery was 97%, respiratory rates 99/ min, heart pulse was detected as179/min. The mean saturation value of the subjects in the second group were 96%, respiratory rate was 139/min, pulse rate was 237/min, In the third group, the preoperative saturation values were 98%, respiratory rates were 124/min, and pulse rates were 159/min.
The clinical findings of the subjects, the saturation values and respiratory and heart pulse rates, were recorded weekly. Averages of clinical findings and differences between and within groups were assessed by One-way ANOVA and Kruskal-Wallis tests. There was no statistically significant difference between the groups (p = 0.870 and p = 0.514 respectively).
There was a significant difference between the groups only in the saturation levels at first week. In the Kruskal-Wallis test, the mean saturation levels of the third group (early fixation group) were statistically better than the other groups (p = 0.032) (Table 2).
CBC (Hgb, Hct, WBC, RBC and PLT counts) and ABG (pH, pO2, pCO2, cHCO3, cHB, sO2, cK, cNA, cCA, cGlu, cLac, cBil) analyzes of subjects were evaluated by Kruskal-Wallis and Wilcoxon tests. There was no statistically significant difference between preoperative and postoperative results (p = 0.165-1.00).
Discussion
In our study, the differences between the postoperative first week saturation levels were statistically significant (p = 0.032). Group III’s (early fixation model) results were better than the other groups. Similar results were obtained in studies in the literature. Preoperative and postoperative results of patients who underwent rib fixation due to flail chest were compared for saturation values, decrease in incidence of pneumonia, time to return to normal life, FVC values, chest wall function and cosmetic appearance were found to be better who underwent surgery [14-17].A clinically significant result in our study was the survival of the subjects. A three-week survival analysis, in which subjects were assumed to live at least one day; mean survival in the group III (early fixation) was better than the other groups. Although survival rates were clinically significant in the group III (early rib fixation), the differences between the groups were not statistically significant (p = 0.750, p = 0.224, p = 0.402 respectively)
It was seen that the subjects in the group III returned to their normal eating and drinking habits during at the first week. They were more active, and it is observed that they had less pain than the others. We think the health status of the group III is better than the other groups. There are texts in the literature recommending rib fixation to reduce the pain of the patient if the fracture ends are moving in multiple and displaced rib fractures, even if they do not have flail chest [18].
We observed that displaced rib fractures did not heal properly due to the penetration of connective tissue between the fractured ends. This also caused a deformity in the chest wall.
There are also disagreements about the timing of the surgical treatment. Some authors performed surgical treatment within 36-48 hours after trauma, some have undergone surgical treatment on the fifth day of trauma [14,15]. But common view among authors is that surgery should not be applied when there is contusion in the lung, head trauma or major organ injury after trauma [13,19].
According to some authors, early-stage surgery causes removal of the hematoma in the fracture line and delays in fracture healing [20,21]. In a study on rabbits, it was indicated that the callus in the fractured area of the subjects which had been fixed on the 10th day after trauma was more stable [22]. However, in our study, it was observed that fracture healing was better in the early fixation group.
In conclusion, considering today’s operative techniques and minimally invasive approaches, in patients with multiple and displaced rib fractures without lung contusion and major organ injury, it is appropriate to perform rib fixation surgery before complications occur.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Reference
1) Guitron J, Huffman LC, Howington JA, LoCicero III J. Blunt and Penetrating Injuries of the Chest Wall, Pleura, and Lungs. Içinde: General Thoracic Surgery 7th Edition. 2009. s. 891–902.
2) LoCicero J, Mattox KL. Epidemiology of chest trauma. Surg Clin North Am. 1989; 69: 15-9.
3) Khandhar SJ, Johnson SB, Calhoon JH. Overview of thoracic trauma in the United States. Thorac Surg Clin. Elsevier; 2007; 17: 1-9.
4) Chan O, Hiorns M. Chest trauma. Eur J Radiol 1996; 23: 23-34.
5) Kemmerer W. Patterns of thoracic injuries in fatal traffic accidents. J Trauma 1961; 1: 595-9.
6) Conn J, Hardy J. Thoracic trauma: analysis of 1022 cases. J Trauma 1963; 3: 22-40.
7) Bergeron E, Lavoie A, Clas D, Moore L, Ratte S, Tetreault S, et al. Elderly trauma patients with rib fractures are at greater risk of death and pneumonia. J Trauma 2003; 54: 478-85.
8) Wilson RF, Murray C, Antonenko DR. Nonpenetrating thoracic injuries. Surg Clin North Am 1977; 57: 17-36.
9) Garcia VF, Gotschall CS, Eichelberger MR, Bowman LM. Rib fractures in children: a marker of severe trauma. J Trauma 1990; 30: 695-700.
10) Marasco S, Liew S, Edwards E, Varma D, Summerhayes R. Analysis of bone healing in flail chest injury. J Trauma Acute Care Surg 2014; 77: 452-8.
11) Nirula R, Diaz JJ, Trunkey DD, Mayberry JC. Rib fracture repair: Indications, technical issues, and future directions. World J Surg 2009; 33: 14-22.
12) Mayberry JC, Ham LB, Schipper PH, Ellis TJ, Mullins RJ. Surveyed opinion of American trauma, orthopedic, and thoracic surgeons on rib and sternal fracture repair. J Trauma 2009; 66: 875-9.
13) Lube MW. Surgical fixation of rib fractures. 2013; 1–8. Updated June 02, 2013. Accessed December 19, 2017.http://www.surgicalcriticalcare.net/Guidelines/ Surgical%20 Fixation%20of%20Rib%20Fractures%202013.pdf .
14) Granetzny A, Abd El-Aal M, Emam E, Shalaby A, Boseila A. Surgical versus conservative treatment of flail chest. Evaluation of the pulmonary status. Interact Cardiovasc Thorac Surg 2005; 4: 583-7.
15) Tanaka H, Yukioka T, Yamaguti Y, Shimizu S, Goto H, Matsuda H, et al. Surgical stabilization of internal pneumatic stabilization? A prospective randomized study of management of severe flail chest patients. J Trauma 2002; 52: 727–732; discussion 732.
16) Ahmed Z, Mohyuddin Z. Management of flail chest injury: Internal fixation versus endotracheal intubation and ventilation. J Thorac Cardiovasc Surg 1995; 110: 1676–80.
17) Beal SL, Oreskovich MR. Long-term disability associated with flail chest injury. Am J Surg 1985; 150: 324-6.
18) Girsowicz E, Falcoz PE, Santelmo N, Massard G. Does surgical stabilization improve outcomes in patients with isolated multiple distracted and painful non-flail rib fractures? Interact Cardiovasc Thorac Surg 2012; 14: 312-5.
19) Voggenreiter G, Neudeck F, Aufmkolk M, Obertacke U, Schmit-Neuerburg KP. Operative chest wall stabilization in flail chest - Outcomes of patients with or without pulmonary contusion. J Am Coll Surg 1998; 187: 130-8.
20) Grundnes O, Reikerås O. The importance of the hematoma for fracture healing in rats. Acta Orthop Scand 1993; 64: 340-2.