



Summary
Chest wall tumors may originate from the skin, muscles, adipose tissue, nerves and blood vessels, bone and cartilage tissue. Primary malignant tumors of the chest wall are rare. When contextualized, soft tissue stands out as the major origin of primary chest wall tumors. Lipomas, one of the most common benign soft tissue lesions, may mimic malignant masses with their clinical and radiological manifestations. We aimed to present a case of giant lipoma with the complaint of severe pain with the review of the literature.Introduction
Chest wall tumors encompass various tumors of the musculoskeletal system forming the chest wall. Metastatic tumors account for more than half of chest wall tumors. Primary malignant chest wall tumors originate from soft tissue, cartilage and bone tissue [1]. Primary chest wall tumors represent less than 1-2% of all malignancies [2]. Among the primary malignant chest wall tumors, about 55% originate from cartilage and bone tissue, while 45% originate from soft tissue [3]. The most common malignant chest wall tumors are malignant fibrous histiocytoma, chondrosarcoma and fibrosarcoma, while the most common benign chest wall tumors are chondroma, lipoma and fibroma [4].Lipomas, one of the most common benign soft tissue lesions, may mimic malignant masses with their clinical and radiological manifestations. They rarely exhibit excessive growth and can be termed as giant lipoma, if they are greater than 10 cm in diameter. With their slow growth, well-encapsulated and mobile characteristics, lipomas can be differentiated from other tumoral formations based on clinical findings, and they may be present in the breast tissue.
Case Presentation
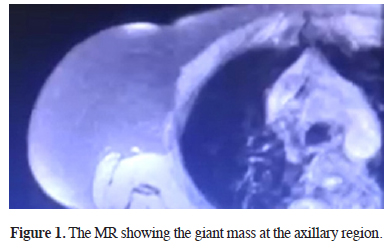
A 61-year-old male patient admitted to the hospital with complaint of a lump in his chest wall. He recognized it 3 years previously and chest pain increased parallel to the progressive enlargement. The physical examination revealed an oval, mobile soft mass lesion in the right hemithorax. The magnetic resonance (MR) of thorax showed a well-demarcated soft tissue lesion with multiple septations extending into the right paracostal muscle structures. The mass was predominantly located under the latissimus dorsi muscle on the right chest wall. The lesion did not cause destruction in the costa and had no relationship with the right hemothorax (Figure 1).){kind=link}
 Click Here to Zoom |
Figure 1: The MR showing the giant mass at the axillary region. |
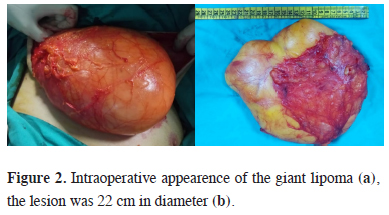
Since the possibility of malignancy could not be eliminated on the examinations carried out, surgical intervention was planned for diagnosis and treatment. The patient was placed in the right posterolateral position and via a 10 cm incision across the right anterior axillary and nipple line, which was above the fifth costa, the mass was observed under latissimus dorsi muscle, and excised totally. No costal invasion was present (Figure 2). Histolopathologic examination confirmed lipoma.
){kind=link}
 Click Here to Zoom |
Figure 2: Intraoperative appearence of the giant lipoma (a), the lesion was 22 cm in diameter (b). |
The patient was discharged on the third postoperative day uneventfully.
Discussion
Chest wall tumors grow slowly and do not show symptoms in the first stage. However, as the tumor grows, they begin to manifest symptoms. Especially malignant chest wall tumors are more symptomatic. Pain and swelling are the most common symptoms. Lipoma is a slow-growing, benign, painless, mobile, oval and round soft tissue tumor. Although lipoma arises in all age groups, it typically occur in adults aged from 40 to 60 years. In general, it is identified in the subcutaneous tissue of the back, shoulder, head and neck. The skin overlying the lesion appears normal. It is easily detected on physical examination, usually does not require treatment. This tumor may also be found in deep tissues such as the thorax, intra-abdominal organs and intermuscular septae [5,6]. They rarely exhibit excessive growth and can be called giant lipoma, if they grow greater than 10 cm in diameter. With their slow growth, well-encapsulated and mobile characteristics, lipomas can be differentiated from other tumoral formations based on clinical findings, and they may also be present in the breast tissue [7]. Besides conventional radiology, CT is also important for the diagnosis of chest wall tumors. Especially in the diagnosis of neural tumors, magnetic resonance imaging is very important in determining the relationship of the tumor with vascular structures and mediastinum. In addition to chest x-ray, CT was performed on our patient. On CT, lipoma is usually visualized as a well-demarcated mass consisting of almost completely mature adipose tissue. This imaging technique also shows the lesion related invasion in adjacent tissues. In chest wall tumors, it may be clinically and radiologically challenging to differentiate whether the lesion is benign or malignant. Needle aspiration, incisional biopsy or excisional biopsy can be used in the diagnosis of these tumors. However, needle aspiration and incisional biopsy may cause the tumor to spread along the biopsy tract. Therefore, as far as possible, complete resection of the tumor and making a definitive diagnosis should be ensured. In cases with suspicious surgical margin, the analysis of frozen sections is absolutely necessary. Considering the advanced growth of the mass and inevitable total excision due to its location in the case, surgical resection was carried out without considering the surgical biopsy methods, and the definitive diagnosis and treatment were provided. The histopathological examination of the mass was reported as giant lipoma.In conclusion, lipomas, which are most commonly benign soft tissue lesions of the chest wall, can mimic malignant masses with clinical and radiological manifestations. Surgical interventions and pathological examinations performed for definitive diagnosis may bring surprising results. Especially in cases of ignored pain and swelling, necessary diagnostic procedures should be performed promptly, and large resection should not be avoided in operable cases.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support
Reference
1) Incarbone M, Pastorino U. Surgical treatment of chest wall tumors. World J Surg 2001; 25: 218–30.
2) Ozpolat B, Ozeren M, Akkaya T, Yucel E. Giant lipoma of chest wall. Eur J Cardiothorac Surg 2004; 26: 437.
3) Incarbone M, Pastorino U. Surgical treatment of chest wall tumours. World J Surg 2001; 25: 218-30.
4) Pairolero PC. Chest wall tumours. In Shields TW, LoCicero J, Poon RB, eds. General Thoracic Surgery. Philadelphia: Lippincott Williams&Wilkins, 2000; 589-98.
5) Salam GA. Lipoma excision. Am Fam Physician 2002; 65: 901-4.