



Summary
Hydatid cyst is a parasitic disease caused by Echinococcus cestode. Hydatid cyst is an important risk factor in rural areas especially in Mediterranean countries, Middle East and Australia. The disease is most common in the liver and then in the lungs and it is very rare to be seen primarily in the chest wall. We present a 31 years-old female patient with primary chest wall hydatid cyst and discuss the surgical treatment.Introduction
Hydatid cyst is a zoonotic parasitic disease and Echinococcus granulosus is frequently responsible for this disease [1]. In Turkey, the incidence of hydatid cyst is 2000-2500 cases per year [2]. Cyst formation is the most seen in the liver and it is followed by the lung with a percentage of 10-30% [3]. Although the disease can be seen in different of the body like spleen, kidney, orbit, heart and brain, chest wall is very uncommon localization for this disease [4,5]. This paper is a case report of a 31 years-old female patient with chest wall hydatid cyst without any other organ system involvements.Case Presentation
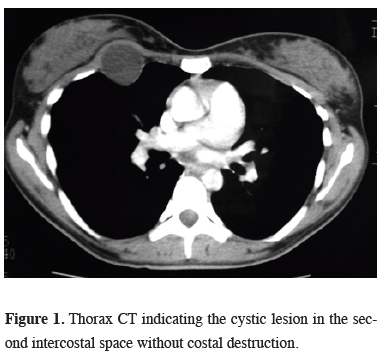
A 31 years-old female patient admitted to the hospital with complaints of chest pain and a mass on the right hemithorax. Physical examination revealed a 4 cm mass on the right chest wall. Thorax computed tomography (CT) revealed a cystic lesion with a diameter of 4x3 cm on the third intercostal space of the right hemithorax without costal destruction (Figure 1).){kind=link}
 Click Here to Zoom |
Figure 1: Thorax CT indicating the cystic lesion in the second intercostal space without costal destruction. |
Surgical excision was planned for the exact diagnosis and the treatment. A thoracic incision was made through the third intercostal space, and after dissection of the subcutaneous tissue and pectoral muscles, a cystic lesion of 4x4 cm diameter was visualized between the muscles of intercostal region that was fluctuating on palpation. The ribs were not invaded and the cystic lesion was bulging through the intrapleural space. It was totally excised with blunt and sharp dissection. Cuticular membrane of cystic lesion was confirmed on the specimen. There was no complication postoperatively. Histopathologic examination confirmed that the lesion was hydatid cyst. Albendazole was administered after the operation. The patient was discharged on day 5 uneventfully.
Discussion
Although there are several studies about chest wall hydatid cysts in the literature, primary chest wall involvement is very rare and in most of the patients chest wall was reported to be the secondary place of hydatid disease following the other system involvements [4-6]. In this case, chest wall was considered to be the primary location for the hydatid cyst because no sign of disease was detected elsewhere.To distinguish of chest wall hydatid cyst from other masses is difficult, as primary chest wall involvement of hydatid disease cannot be considered first by physicians. Chest radiographs usually show us unruptured cysts as round homogeneous well-defined densities but like in the patient reported by Demir et al. the disease can destruct the ribs and can mimic a chest wall tumor [7]. Also CT is not pathognomonic in these patients.
In patients with a history of surgery for lung hydatid cyst, masses of the thoracic wall must be considered as the spread the disease to the chest wall [5]. The pulmonary cysts may rupture spontaneously or during surgery. Rupture of the pulmonary hydatid cysts into the pleural space may contaminate the adjacent organs and this may result to development of pleural or chest wall hydatid cysts. Likewise, in patients with concomitant cystic lesions especially in the lung and liver with the cystic chest wall masses may be considered as clues of the chest wall hydatid cyst. Although in our patient we did not detect a clue considering hydatid cyst, we decided surgery because it would be appropriate for the diagnosis and treatment of this type of cystic lesions of the thoracic wall. In our opinion, percutaneous biopsy is not suitable in such patients due to the risk of rupture of the cyst and dissemination of the infection.
In this case, the intercostal involvement is via systemic circulation i.e. to right heart after passing the common sites, liver and lung. The involvement of body’s unexpected portions can be seen rarely with systemic circulation of hydatid cyst [1].
Surgical treatment of the disease is radical removal of involved chest wall. In this case, only the intercostal muscle was involved, therefore the cyst and muscle around it were totally excised. Medical treatment should be used after surgery to avoid recurrences. Albendazole treatment after surgery has a high response rate without recurrence [8]. There are studies that albendazole should be used preoperatively [9]. Although preoperative albendazole treatment can sterilize cyst cavity, it can also cause rupture of the intact cyst and may cause further complications.
In conclusion, hydatid cyst must be considered in the differential diagnosis of chest wall masses when dealing with chest wall tumors even without apparent risk factors. Appropriate treatment of primary chest wall hydatid cyst is surgical excision.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Reference
1) Harlaftis NN AH, Symbas PN. Hydatid disease of the lung. In: Shields TW LJ, Ponn RB, Rusch VW, editor. General Thoracic Surgery 6ed. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 1298-07.
2) Altintas N. Past to present: echinococcosis in Turkey. Acta Tropica. 2003; 85: 105-12.
3) Morar R, Feldman C. Pulmonary echinococcosis. Eur Respir J. 2003. 1069-77 p.
4) Oğuzkaya F, Akçali Y, Kahraman C, Emiroğullari N, Bilgin M, Şahin A. Unusually located hydatid cysts: Intrathoracic but extrapulmonary. Ann Thorac Surg 1997; 64: 334-7References
1) Harlaftis NN AH, Symbas PN. Hydatid disease of the lung. In: Shields TW LJ, Ponn RB, Rusch VW, editor. General Thoracic Surgery 6ed. Philadelphia: Lippincott Williams & Wilkins; 2005. p. 1298-07.
2) Altintas N. Past to present: echinococcosis in Turkey. Acta Tropica. 2003; 85: 105-12.
3) Morar R, Feldman C. Pulmonary echinococcosis. Eur Respir J. 2003. 1069-77 p.
4) Oğuzkaya F, Akçali Y, Kahraman C, Emiroğullari N, Bilgin M, Şahin A. Unusually located hydatid cysts: Intrathoracic but extrapulmonary. Ann Thorac Surg 1997; 64: 334-7.
5) Özdemir N, Akal M, Kutlay H, Yavuzer S. Chest Wall Echinococcosis. Chest 1994; 105: 1277-9.
6) Salih AM, Ahmed DM, Kakamad FH, Essa RA, Hunar AH, Ali HM. Primary chest wall Hydatid cyst: Review of literature with report of a new case. Int J Surg Case Rep 2017; 41: 404-6.
7) Demir HA, Demir S, Emir S, Kacar A, Tiryaki T. Primary hydatid cyst of the rib mimicking chest wall tumor: a case report. J Ped Surg 2010; 45: 2247-9.
8) Keshmiri M, Baharvahdat H, Fattahi SH, Davachi B, Dabiri RH, Baradaran H, et al. A placebo controlled study of albendazole in the treatment of pulmonary echinococcosis. Eur Respir J 1999; 14: 503-7.
9) Foroulis CN, Avgoustou C, Konstantinou M, Lioulias AG. Chest wall hydatidosis as the unique location of the disease: Case report and review of the literature. Can J Infect Dis 2003; 14: 167-9..
5) Özdemir N, Akal M, Kutlay H, Yavuzer S. Chest Wall Echinococcosis. Chest 1994; 105: 1277-9.
6) Salih AM, Ahmed DM, Kakamad FH, Essa RA, Hunar AH, Ali HM. Primary chest wall Hydatid cyst: Review of literature with report of a new case. Int J Surg Case Rep 2017; 41: 404-6.
7) Demir HA, Demir S, Emir S, Kacar A, Tiryaki T. Primary hydatid cyst of the rib mimicking chest wall tumor: a case report. J Ped Surg 2010; 45: 2247-9.