



Summary
Modified Ravitch procedure is the hallmark surgical procedure to repair pectus deformities, manual and auto self-retaining metal retractors are very helpful because they grant and maintain the surgical site exposure. However, these metal retractors often have sharp tips that are capable of causing soft tissue flaps damage. In abdominal surgery, using an atraumatic O-ring wound retractor has been associated with diminution of superficial surgical site complications and post-operative pain reduction due, these suggested benefits can be reproducible in modified Ravitch procedure. A 20-year-old male patient is referred to our service for presenting chest discomfort and body image issues. Subsequent work up revealed a pectus carinatum without associated congenital heart disease. A transverse infra-mammary skin 8 cm incision was made. We used an atraumatic O-ring wound retractor to expose surgical site and performed bilateral subperichondrial abnormal costal cartilages resection with sternum wedge osteotomy. Drains was removed in 24 hours, and the post-surgical hospital stay was 72 hours. In this case, using an atraumatic O-ring wound retractor improved exposure with shorter incision, facilitated stable access to the costal cartilage, protecting the skin from injury, and reduced the administration of intravenous analgesics.Introduction
Modified Ravitch procedure is the open surgical procedure of choice to repair pectus deformities [1]. The approach can be performed with a transverse or vertical 10 cm incision. Skin and muscle flaps are made elevating pectorals muscles to expose the sternum and bilateral costal cartilages [1,2]. To carry out the surgical correction surgeon hand retractors are used to expose the surgical field, The way it pulls and the force applied cause soft tissue damage [3]. Enhanced recovery program (ERP) is an evidence-based multidisciplinary approach to optimize the recovery of surgical patients in colorectal surgery. Lohsiriwat in 2014 identified soft tissue damage as a comorbid factor that intensifies post-operative pain and cause cicatrisation outcome alteration [3,4]. In 2012 Cheng and Biewenga reported that atraumatic O-ring retractor is a modern self-retaining wound retractor which provides circumferential retraction that causes less tissue damage, thus reducing pain following open surgeries than conventional auto self-retractors [4-6]. Modified Ravitch procedure has been associated to soft tissue complications due extensive dissection and prolonged intravenous analgesia administration for pain management [1,2]. In this case report we describe the use of an atraumatic O-ring wound retractor for modified Ravitch procedure in order to obtain the benefits of the atraumatic device in the thoracic surgery field.Case Presentation
A 20-year-old male patient is referred to our service for presenting chest discomfort and body image issues. Subsequent work up revealed a pectus carinatum without associated congenital heart disease. The patient was operated with general endotracheal anesthesia and placement of a thoracic epidural catheter. A transverse infra-mammary 8 cm incision and soft tissue flaps was performed (Figure 1).){kind=link}
 Click Here to Zoom |
Figure 1: Skin incision and soft tissue flap exposing sternum surgical site. |
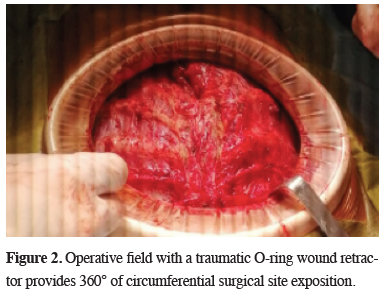
An O-ring wound retractor was used to expose the affected portion of sternum and bilateral costal cartilages (Figure 2).
){kind=link}
 Click Here to Zoom |
Figure 2: Operative field with a traumatic O-ring wound retractor provides 360° of circumferential surgical site exposition. |
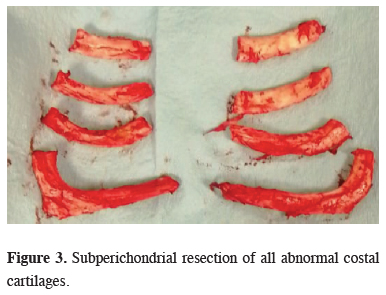
We found a symmetrical anterior protrusion of the body of the sternum with protrusion of the 4, 5, 6 and 7th costal cartilages. Subperichondrial resection of all abnormal costal cartilages was performed (Figure 3), then we performed a wedge osteotomy to neutralize the posterior depression of the sternum.
){kind=link}
 Click Here to Zoom |
Figure 3: Subperichondrial resection of all abnormal costal cartilages. |
Retrosternal and subcutaneous closed drains was placed and soft tissue was closed. Thoracic epidural catheter and drains was removed at 24 hours. Intravenous nonsteroidal anti-inflammatory drugs was switched to oral medication at 48 hours. Patient was discharged under the third post-operative day without complications. Surgery was performed by the thoracic surgery department of Hospital Civil de Guadalajara Fray Antonio Alcalde, Jalisco, Mexico in January 2019.
Discussion
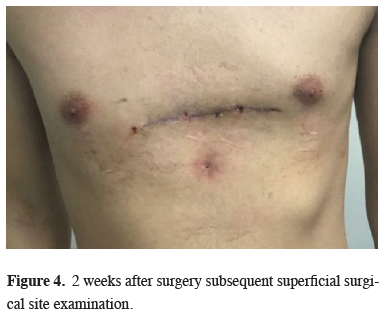
Enhanced recovery program (ERP) identified that tissue damage caused by surgeon hand retractors or metallic conventional self-retaining wound retractor may intensifies post-operative pain and cause cicatrisation outcome alteration [3,4]. Despite the wide dissection needed for soft tissue flaps and the lack of evidence on the utility of the O-ring wound retractor in pectus surgery, we think that its use can avoid soft tissue damage in order to obtain improves in surgical wound management described in abdominal surgery, especially in pain control, and also with the expectative to improve cosmetic scar outcomes. In this case, there were better surgical site exposure that facilitated stable access to costal cartilage resection, protecting the skin from injury during the intervention. We could switch intravenous analgesia to oral intake without the need of opioids with good pain control; this outcome may be attributed by thoracic epidural anesthesia. However we think that the O-ring wound retractor also contributed in pain control, supporting us with Lohsiriwat and Chowdary findings in which they concluded reduction in early postoperative pain and a significant reduction in the amount of intravenous analgesia with the use of an O-ring wound retractor in abdominal surgery [3,6]. The patient was discharged home when the pain was well controlled with oral pain medications (3 days). Subsequent postoperative visit was 2 weeks after surgery without complications (Figure 4), patient referred, no pain, and good satisfaction with the modified Ravitch procedure.){kind=link}
 Click Here to Zoom |
Figure 4: 2 weeks after surgery subsequent superficial surgical site examination. |
In conclusion, there is a lack of high quality/high levels of evidence studies that have been conducted on retractors. However, the outcome most commonly documented in relation atraumatic O-ring wound retractor is a reduction in early postoperative pain and superficial surgical site complications. In this case the use of an atraumatic O-ring wound retractor improved exposure with shorter incision, facilitated stable access to the costal cartilage, protecting the skin from injury, and reduced the administration of intravenous analgesics. Studies are needed to support the use of atraumatic retractors in thoracic surgery field.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Reference
1) Papic JC, Finnell SM, Howenstein AM, Breckler F, Leys CM. Postoperative opioid analgesic use after Nuss versus Ravitch pectus excavatum repair. J Pediatr Surg 2014; 49: 919-23.
2) Hysi I, Vincentelli A, Juthier F, Benhamed L, Banfi C, Rousse N, et al. Cardiac surgery and repair of pectus deformities: When and how? Int J Cardiol 2015; 194: 83-6.
3) Lohsiriwat V, Lohsiriwat D. Atraumatic O-ring wound retractor reduces postoperative pain. Tech Coloproctol 2014; 18: 1177-8.
4) Cheng KP, Roslani AC, Sehha N, Kueh JH, Law CW, Chong HY, et al. Alexis O-Ring wound retractor vs conventional wound protection for the prevention of surgical site infections in colorectal resections. Colorectal Dis 2012; 14: 346-51.