



Summary
Primary mediastinal ectopic goiter (PMG) is defined as the presence of thyroid tissue in the mediastinum without having a continuity between the cervical thyroid and the mediastinal goiter. A fifty-seven yearold man admitted to our clinic suffering from dyspnea, chest pain, shortness of breath, and dysphagia for almost two months. Thorax computed tomography revealed a mass of 12 cm in the posterior mediastinum, compressing the trachea and esophagus. The mass is resected completely via a right thoracotomy.Introduction
Primary mediastinal ectopic goiter (PMG) is briefly defined as the presence of thyroid tissue in the mediastinum; but there are actually four criteria to call a mediastinal thyroid tissue as PMG. There should be a total discontinuity between the cervical thyroid and the mediastinal goiter, presence of blood supply should be from mediastinal vessels, there should be absence of history or evidence of malignancy in both cervical and mediastinal goiter and finally the cervical thyroid gland can be present or absent with no history of thyroidectomy [1]. It constitutes 1% of all mediastinal masses. PMG usually presents itself by causing compression of adjacent structures leading to dysphagia, hoarseness, stridor and symptoms of vena cava superior syndrome [2,3]. Surgical resection is the gold standard for the treatment of PMG.Our aim is to share this rare case and remind that PMG should not be forgotten in differential diagnoses in mediastinal masses.
Case Presentation
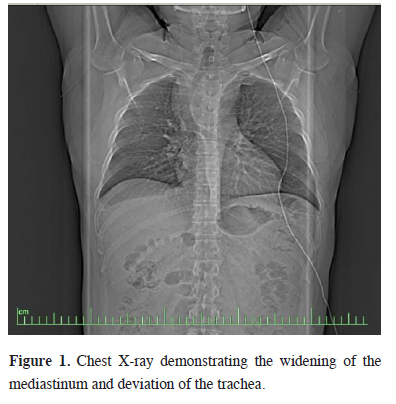
A 57-year-old male patient was referred to our clinic due to dry cough, chest pain, shortness of breath, dyspnea, and dysphagia for three months. Chest X-ray presented a mediastinal widening and a right tracheal deviation (Figure 1).){kind=link}
 Click Here to Zoom |
Figure 1: Chest X-ray demonstrating the widening of the mediastinum and deviation of the trachea. |
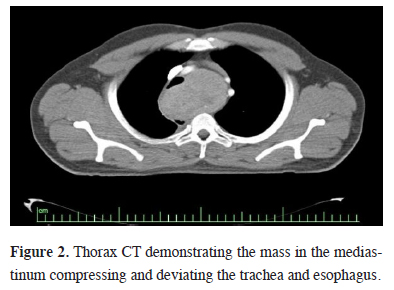
A tracheal shift was evident by palpation during the physical examination. Thorax computerized tomography (CT) revealed a 12x10 cm heterogeneous mass which was located in posterior trachea, adjacent to anterior vertebral column and compressing the esophagus. (Figure 2). Thyroid ultrasonography was normal.
){kind=link}
 Click Here to Zoom |
Figure 2: Thorax CT demonstrating the mass in the mediastinum compressing and deviating the trachea and esophagus. |
He did not have a thyroid operation previously. Routine laboratory tests including thyroid function tests, beta-human chorionic gonadotropin (B-hcg, 0 mıu/ml), alpha-fetoprotein (αFP, 2.2ng/ mL) and lactate dehydrogenase (LDH, 2,2 U/L) were all in normal ranges. Fiberoptic bronchoscopy revealed a severe external compression trachea.
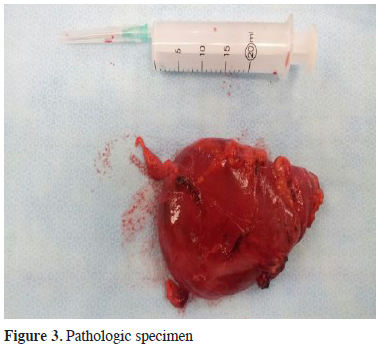
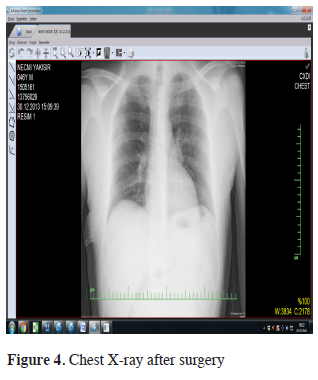
A right lateral thoracotomy is preferred to accomplish a reliable exposure for a posterior mass resection. The mass had no invasions to the adjacent organs and structures and it is resected completely (Figure 3). Histopathologic examination reported macrofolliculer nodular colloidal hyperplasia. Figure 4 shows the postoperative chest x-ray.
){kind=link}
){kind=link}
 Click Here to Zoom |
Figure 3: Pathologic specimen |
 Click Here to Zoom |
Figure 4: Chest X-ray after surgery |
Postoperative course was uneventful and he is under follow-up and disease free for 3 years.
Discussion
Ectopic localization of thyroid tissue is a congenital anomaly which constitutes 1% of all mediastinal masses. Ectopic thyroid tissue may occur in any point along the pathway of migration of primordial thyroid gland from foramen caecum to its final destination, anterior trachea between fourth and eighth week of gestation [2,4]. The anterior mediastinum makes up 75-94% of the localization, while in 10-15% of the cases, they occur in the posterior mediastinum.PMG usually seen in 4th or 5th decades and there is a female preponderance [5]. Although patients are usually asymptomatic and incidentally identified, they may present with symptoms of compression of adjacent organs. Thoracic CT is very sensitive to delineate the nature of the mediastinal masses and their relation to adjacent thoracic structures. Iodine-131 scanning which is used to detect the thyroid tissue in the mediastinal masses, is performed both to investigate the thyroid nature of the mass and to prove that the mass had no relation to cervical thyroid gland.
Thoracic MRI can also be used in addition to thorax CT to plan the surgical approach [6]. βHCG, αFP and LDH levels are essential in the differential diagnosis to distinguish nonseminomatous germ cell tumors from other mediastinal masses. The mass showed a heterogeneous density on CT. Thyroid function tests and βHCG and αFP levels were all normal.
Surgical approach depends on the location of the mass. Median sternotomy, thoracotomy, cervical incision, and thoracoscopy are surgical approaches of PMG resection. In this case we preferred a right lateral thoracotomy due to the localization. The patient was completely symptom free after the resection. After a long term tracheal compression, a postoperative tracheomalacia is a rare but expected complication which was not seen in this case.
In conclusion, this case emphasizes that PMG is a part of differential diagnoses for mediastinal masses despite to its rareness. Thoracotomy is the most common approach to resect mediastinal masses which are greater than 4 centimeter.
Declaration of conflicting interests
The author declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author received no financial support for the research and/or authorship of this article.
Reference
1) Foroulis CN, Rammos KS, Sileli MN, Papakonstantinou C. Thyroid 2009; 19: 213-8.
2) Sakorafas GH, Vlachos A, Tolumis G, Kassaras GA, Anagnostopoulos GK, Gorgogiannis D. Ectopic intrathoracic thyroid: case report. Mt Sinai J Med 2004; 71: 131-3.
3) Mussak EN, Kacker A. Surgical and medical management of midline ectopic thyroid. Otolaryngol Head Neck Surg 2007; 136: 870-2.
4) Noussios G, Anagnostis P, Goulis DG, Lappas D, Natsis K. Ectopic thyroid tissue: anatomical, clinical, and surgical implications of a rare entity. Eur J Endocrinol 2011; 165: 375-82.
5) Sand J, Pehkonen E, Mattila J, Seppanene S, Salmi J. Pulsating mass at the sternum. A primary carcinoma of ectopic mediastinal thyroid. J Thorac Cardiovasc Surg 1996; 112: 833-5.