Discussion
The majority of hydatid cyst diseases are caused by the larval stage of E. Granulosus affecting mostly the liver and lungs, respectively. While the majority of the cases have solitary lesions, there are also cases having multiple lesions. In 60% of the cases, it is located in the right lung and in 20% of the cases the lesions are bilateral [
3,
4]. In all 15 cases included in this study, the lesions were unilateral and solitary and 60% of them were located in the right lung.
Lung hydatid cysts usually are not symptomatic. Symptoms start to appear after the size of the cyst reaches 5 cm and create pressure in the neighboring organs or in the case of ruptured and complicated the cystic lesion [5]. Depending on the size and the localisation of the cyst, non-specific symptoms including cough, hemoptysis and chest pain occur [6]. The most frequent symptoms in the majority of the cases were non-specific ones such as cough, whilst some cases had symptoms such as fever and shivers which could occur after the cyst rupture.
diagnosis of hydatid cyst, tests such as indirect hemagglutination or indirect fluorescent antibody can be applied [7]. However due to the lack of specific diagnosis in the preoperative stage of the cases according to the clinical and radiological findings, serological tests for the diagnosis of hydatid cyst could not be performed. Having said that, despite the positive serological tests for Echinococcus granulosus, there are reports arguing that serological tests, which identify large cell lung carcinoma, can give false positive results [8].
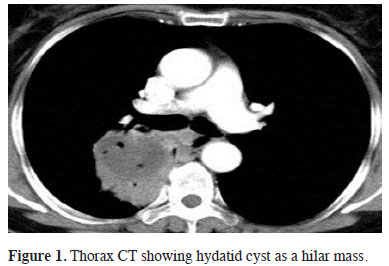
Since the clinical and laboratory findings are not specific in the diagnosis of hydatid cyst, radiological scan gains importance at the diagnosis stage [5]. Cysts that are not complicated are seen as well demarcated round or homogeneous masses in computed tomography and lung graphics. Larger cysts can result in atelectasis in lungs, mediastinal shift or pleural effusion depending on the level of the pressure on the neighbouring tissue. Lung graphics of the complicated cysts can show air-fluid level, water lily or meniscus signs. Ruptured cysts can appear as mass or abscess in computed tomography. Due to the fact that none of our cases had typical radiological findings for hydatid cyst and there were images mimicking abscess or tumour in direct graphics and computed tomography, the diagnostic and surgical approach to the cases showed differences. Five cases that were thought to be malignant were examined in PET-CT and the SUVmax values of these examinations [2-7,8] supported the malignancy diagnosis.
Due to the rise in glucose metabolism in the malignant pulmonary nodules, the FDG retention in the nodule also shows an increase. Lesions with FDG retention with SUVmax value higher than 2.5-3 in PET-CT are usually evaluated as malign [9]. However, as a result of rise in FDG retention due to infection and granulomatosis and inflammation, false positive results are not unexpected. The most frequent false positive results are seen in diseases including tuberculosis, sarcoidosis, aspergillus and parasitary diseases [10]. Local inflammation caused by cyst rupture in our cases resulted in positive PET-BT results for malignancy. Similar to our study, there are reports on breast carcinoma cases which were initially evaluated as pulmonary metastatic lesion in PET-CT and later was diagnosed as hydatid cyst during the surgical stage [11], or cases which underwent surgery due to the lesion which showed pulmonary hypermetabolic retention in PET-CT but later diagnosed as infected consolidated hydatid cyst during the pathological examination [12]. In another study conducted on this issue, it was reported that hydatid cyst disease can easily be confused with thoracic empyema, mediastinal mass, tuberculosis pleurisy and thoracic wall tumour [13].
As a conclusion it should be kept in mind that pulmonary hydatid cyst in endemic regions clinically and radiologically can mimic lung cancer and lung abscess.
Declaration of conflicting interests
The author declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The author received no financial support.







){kind=link}
){kind=link}
){kind=link}
){kind=link}