



2Department of Thoracic Surgery, Edirne Sultan 1. Murat State Hospital, Edirne, Turkey
3Department of Public Health, Trakya University, Edirne, Turke
4Department of Thoracic Surgery, Manisa Celal Bayar University, Manisa, Turkey
5Department of Radiology, Izmir Katip Çelebi University, Izmir, Turkey DOI : 10.26663/cts.2024.023
Summary
Background: Background: Rib fractures rank among the most common conditions in thoracic traumas. Chest radiography is often insufficient for diagnosing rib fractures. Therefore, the study aimed to evaluate the success of thoracic ultrasonography (US) in diagnosing rib fractures.Materials and Methods: Patients over 18 years of age who were hospitalized in our clinic due to traumarelated rib fractures between 2022 and 2023, were included. All patients had chest radiography and computed tomography (CT) scans during their emergency admission, as per the routine operation of the emergency department. Chest radiography and CT images were evaluated by the thoracic surgery clinic, and CT images were also examined through the radiology reports. Thoracic US was performed on all patients by the same radiologist the day after admission to the clinic. The patient's demographic characteristics, chest radiography, chest CT, and thoracic US findings were recorded, and the data were compared statistically.
Results: A total of 58 cases were included in the study, 42 (72.4%) males and 16 (27.6%) females. The mean age of the study population was 60.55 ± 15.71 years. When evaluated regarding trauma types, 42 (72.4%) patients had a fall, 15 (25.9%) had a traffic accident, and 1 (1.7%) patient had a history of battery. In addition to rib fractures, hemothorax was detected in 67.2% of the cases, pneumothorax in 27.6%, and pulmonary contusion in 19.0%. In radiological imaging, while 246 rib fractures were reported according to CT, 136 rib fractures were detected in USG and 140 in direct radiography. Considering CT imaging is the gold standard, 114 of 246 rib fractures (46.3%) could be detected with ultrasound imaging, while 127 (51.6%) were determined with direct radiography.
Conclusions: When chest CT is considered the gold standard, direct radiography, and thoracic US have no general superiority over each other.
Introduction
Trauma is the third most common cause of death among all deaths and the most common in people over the age of 40 [1]. A rib fracture is the most frequent skeletal system pathology in blunt thoracic trauma. It occurs in approximately 25% of blunt thoracic traumas [2,3]. The most commonly used diagnostic methods for diagnosing rib fractures are physical examination and chest radiography; approximately 49% of rib fractures can be detected with these methods. Nevertheless, fractures, especially those occurring in the costal cartilage, cannot be determined by chest radiography [2-4]. This situation causes some rib fracture diagnoses to be overlooked with direct radiography.In thoracic traumas, computed tomography (CT) is a superior examination compared to plain radiography in evaluating chest wall pathologies [5]. This approach allows for revealing almost all trauma-related conditions with detailed images. However, in trauma patients, CT is an appropriate examination only for hemodynamically stable patients, as the patient is separated from the trauma team during the imaging [6]. In addition, there are disadvantages, such as high radiation intake for pregnant patients and high cost [5]. Thus, thoracic ultrasonography (US) is sometimes used as an alternative to chest CT [7]. Although ultrasonography is not widely used to diagnose traumatic rib fractures, various studies have been conducted in the literature [2,3,8,9].
This study aimed to determine the effectiveness of ultrasonography in diagnosing rib fractures by comparing chest CT, thoracic US, and plain radiography results in trauma patients.
Methods
Patients over the age of 18 who were hospitalized in our clinic due to trauma-related rib fractures between October 20, 2022, and July 01, 2023, were included in the study. All patients included in the study had chest radiography and chest computed tomography (CT) during their emergency admission, as per the routine operation of our emergency department. Chest radiography and CT images were evaluated by the thoracic surgery clinic, and CT was also assessed through the radiology reports. Thoracic US was performed on all patients by the same radiologist the day after admission to the clinic. The radiologist was not informed about the patient's clinic or other imaging findings. The patients' demographic information, chest radiography, CT, and thoracic US findings were recorded, and the data obtained was compared statistically. Our study was conducted with decision number 2019/45 of Balıkesir University Clinical Research Ethics Committee.
Statistical Analyses
The data obtained were analyzed statistically using the
SPSS program (Statistical Package for the Social Sciences
Version 22.0; SPSS Inc. Chicago, IL, USA). Categorical
data were presented as numbers (n) and percentages
(%), and continuous data as mean ± standard
deviation (SD) values. Sensitivity, specificity, negative
predictive value, positive predictive value, and accuracy
calculations were calculated with 95% confidence
intervals using the MedCalc program (MedCalc Software
Ltd- version 20.015).
Results
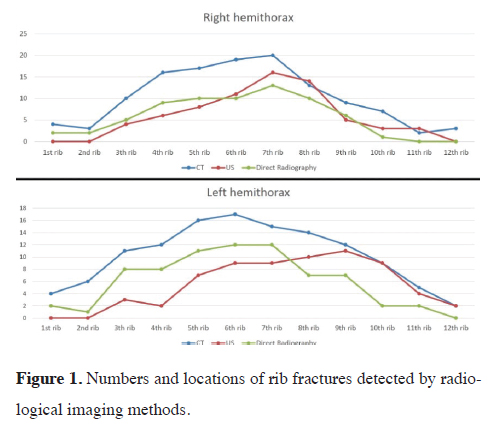
A total of 58 cases were included in the study, 42 of which (72.4%) were male and 16 (27.6%) were female. The mean age of the cases was 60.55 ± 15.71 years. When the symptoms were examined, it was observed that 51 patients (87.9%) had only chest pain complaints, while 7 (12.1%) had chest pain with shortness of breath. When evaluated regarding trauma types, 42 (72.4%) patients had a fall, 15 (25.9%) had a traffic accident, and 1 (1.7%) patient had a battery history. In addition to rib fractures, hemothorax was detected in 67.2% of the cases, pneumothorax in 27.6%, and pulmonary contusion in 19.0%. The numbers and locations of rib fractures detected in the cases according to the data obtained from all three radiological examinations are presented in Figure 1.){kind=link}
 Click Here to Zoom |
Figure 1: Numbers and locations of rib fractures detected by radiological imaging methods. |
In radiological imaging, while 246 rib fractures were reported according to CT, 136 rib fractures were detected in USG and 140 in direct radiography. Considering CT imaging is the gold standard, 114 of 246 rib fractures (46.3%) could be detected with ultrasound imaging, while 127 (51.6%) were determined with direct radiography. Of the 246 rib fractures, 123 (50.0%) were observed in the right hemithorax and 123 (50%) in the left hemithorax. The distribution and relationship analysis of rib fractures detected by USG and direct radiography according to CT results are summarized in Tables 1 and 2.
){kind=link}
){kind=link}
Table 1. Distribution of rib fractures detected on US and direct radiography compared to CT results.
Table 2. Validity analysis of US and direct radiography according to CT results.
The evaluations revealed that the first and second rib fractures in both the right and left hemithorax could not be visualized with thoracic US. It was observed that chest CT detected significantly more rib fractures, especially between the 4th and 9th ribs, where traumatic rib fractures are most common. We determined that direct radiography and thoracic US could detect fewer rib fractures than CT, but they did not have a significant advantage over each other.
Considering chest CT as the gold standard in diagnosing rib fractures, the sensitivity of thoracic US was 46.34%, while the sensitivity of direct radiography was 51.63%. The specificity was determined to be 31.25% for thoracic US and 59.38% for direct radiography. Rib fractures were further grouped according to their locations as anterior, posterior, and lateral, and validity analyses of US and direct radiography were performed by excluding cases with multiple localizations from the analysis (Table 3).
){kind=link}
Table 3. Validity analysis of US and direct radiography according to fracture location.
Discussion
One of the most common pathologies in blunt thoracic trauma is rib fractures. The imaging methods commonly used in our country to diagnose rib fractures are direct radiography and chest CT. The literature review has revealed that thoracic direct radiography is the first imaging choice in cases of blunt chest trauma, and it is recommended by the American College of Surgeons Committee (ACSC) [10,11]. Przerwa et al have reported in their study that chest CT is superior to radiography in revealing injuries due to chest trauma [1]. In this study, they made changes in treatment management after chest CT in 83% of the patients. Jin et al also demonstrated in their study that low-dose CT imaging was satisfactorily successful in the diagnosis of rib fractures [12]. While chest radiography and CT are primarily used as imaging in the approach to trauma patients, bedside US imaging may be required in pregnant patients, unstable patients who cannot be transferred to the imaging unit, and patients with mental problems who cannot lie still during imaging. The authors planned the present study based on this idea.In their study, Schellenberg et al [10] determined the chest CT method as the gold standard method to compare imaging methods in evaluating thoracic traumas. In our study, we also considered the chest CT method as the gold standard method when determining the effectiveness of US in the diagnosis of rib fractures. However, there were also rib fractures that we observed on US or radiography that could not be determined on CT. Sano et al compared chest CT and radiography in their study. In their study of 75 patients, they were able to detect the same rib fractures in 56% of the patients with both chest CT and radiography. Of the 217 rib fractures detected in their study, they could not observe rib fractures in 43 patients with chest radiography and in 21 with chest CT [13].
Turk et al evaluated 20 patients with blunt chest trauma with thoracic US who were symptomatic, but no pathology was determined on chest radiography [3]. In 18 of these patients, 26 rib fractures were detected, and thoracic US was demonstrated to be more sensitive than radiography. In their review, Battle et al stated that the thoracic US was more sensitive than chest radiography in diagnosing rib fractures, but there was a risk of bias in the studies included [14]. Similarly, a meta-analysis published by Yousefifard et al concluded that thoracic US was superior to chest radiography in diagnosing rib fractures, particularly if the US was performed by a radiologist [15]. The study performed by Hwang and Lee emphasized that the thoracic US was an effective method in diagnosing rib fractures, but the results obtained were insufficient to indicate that it was a more effective examination compared to direct radiography [16]. Pishbin et al performed thoracic US and chest radiography on 61 blunt thoracic trauma patients and detected a total of 59 rib fractures in 38 of these patients [2]. While they detected 58 of 59 rib fractures in 38 patients with thoracic US, they could not observe a rib fracture behind the scapula. However, they were able to detect 32 rib fractures in only 20 patients out of 59 rib fractures with chest radiography. In their study, thoracic US specificity was 100%, and sensitivity was 98.31%, while chest radiography had a specificity of 100% and sensitivity of 40.68%. Since chest CT was not used in the evaluation, their specificity and sensitivity rates were relatively high. In our study, since chest CT was used and considered this imaging method the gold standard, we determined the specificity of US to be 31.25%, its sensitivity to be 46.34%, and the specificity of radiography to be 59.38%, and sensitivity to 51.63%. In this study, unlike others, the effectiveness of thoracic US was demonstrated to be lower than radiography. We believe that the most crucial reason for this result was that the use of US in thoracic trauma and rib fracture is not commonly accepted by radiologists and their reluctance towards the procedure.
The most critical limitation of our study was convincing the radiologists to study the role of US in rib fractures. Since trauma patients are evaluated with chest radiography and CT in routine practice, thoracic US was not willingly performed by the radiology clinic. The study could be conducted with only one radiology doctor who was persuaded to participate. This condition caused the number of patients included in our study to be limited.
In conclusion, the present study indicated that chest CT was much superior to direct radiography and thoracic USG in diagnosing rib fractures. When chest CT is considered the gold standard, direct radiography, and thoracic US have no general superiority over each other. Thus, considering the conditions of our country, although radiography is still the first choice due to its easy accessibility, thoracic US can also be used in special patients or conditions.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect
to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research
and/or authorship of this article.
Ethics approval
The study was approved by of Balıkesir University
Clinical Research Ethics Committee. (Date/Number:
2019/45)
Authors’ Contribution
MK; designing the study, collection of data, interpreting
the analyzed data, reviewing the literature, writing and
editing of the study, İA; design of the study, ACY; analyzing
the data, interpreting the analyzed data, reviewing
the literature, writing the study, AA; Writing and
editing of the study, CC, NBS, EBŞ; collection of data.
All authors read and approved the final manuscript.
Reference
1) Błasińska-Przerwa K, Pacho R, Bestry I. The application of
MDCT in the diagnosis of chest trauma. Pneumonol Alergol
Pol 2013; 81: 518-6.
2) Pishbin E, Ahmadi K, Foogardi M, Salehi M, Seilanian Toosi F,
Rahimi-Movaghar V. Comparison of ultrasonography and radiography
in diagnosis of rib fractures. Chin J Traumatol 2017;
20: 226-8.
3) Turk F, Kurt AB, Saglam S. Evaluation by ultrasound of traumatic
rib fractures missed by radiography. Emerg Radiol 2010;
17: 473-7.
4) Crandall J, Kent R, Patrie J, Fertile J, Martin P. Rib fracture
patterns and radiologic detection a restraint-based comparison.
Annu Proc Assoc Adv Automot Med 2000; 44: 235-59.
5) Deunk J, Dekker HM, Brink M, van Vugt R, Edwards MJ, van
Vugt AB. The value of indicated computed tomography scan of
the chest and abdomen in addition to the conventional radiologic
work-up for blunt trauma patients. J Trauma 2007; 63: 757-63.
6) Reuter M. Trauma of the chest. Eur Radiol 1996; 6: 707-16.
7) Weingrow D. Under what situations is ultrasound beneficial for
the detection of rib fractures? Ann Emerg Med 2022; 79: 540-2.
8) Hurley ME, Keye GD, Hamilton S. Is ultrasound really helpful
in the detection of rib fractures? Injury 2004; 35: 562-6.
9) Çelik A, Akoglu H, Omercikoglu S, Bugdaycı O, Karacabey S,
Kabaroglu KA et al. The diagnostic accuracy of ultrasonography
for the diagnosis of rib fractures in patients presenting to
emergency department with blunt chest trauma. J Emerg Med
2021; 60: 90-7.
10) Schellenberg M, Inaba K, Bardes JM, Orozco N, Chen J, Park
C et al. The combined utility of extended focused assessment
with sonography for trauma and chest x-ray in blunt thoracic
trauma. J Trauma Acute Care Surg 2018; 85: 113-7.
11) Trauma ACoSCo. Thoracic trauma. Advanced trauma life support
(ATLS), 9th ed. Chicago: Hearthside Publishing Services; 2012.
12) Jin L, Ge X, Lu F, Sun Y, Li C, Gao P et al. Low-dose ct examination
for rib fracture evaluation: A pilot study. Medicine
2018; 97: e11624.
13) Sano A. Rib radiography versus chest computed tomography
in the diagnosis of rib fractures. Thorac Cardiovasc Surg 2018;
66: 693-6.
14) Battle C, Hayward S, Eggert S, Evans PA. Comparison of the use
of lung ultrasound and chest radiography in the diagnosis of rib
fractures: A systematic review. Emerg Med J 2019; 36: 185-90.