



2Department of Thoracic Pathology, Faculty of Medicine, Suleyman Demirel University, Isparta, Turkey DOI : 10.26663/cts.2025.006
Summary
Chest wall hamartoma is a rare pathology in adults, usually presenting at birth or in early infancy. They may present with compression symptoms depending on their localization. Although it is rare to be recognized with late-onset symptoms in adults, it requires differential diagnosis with other malignant and benign tumors of the chest wall. Histologically, carcinoid tumors are classified into two subgroups as typical and atypical. Atypical carcinoids have an aggressive course and have the potential for metastasis and recurrence. Typical carcinoids are low grade malignancies. Although the prognosis of carcinoid tumors after surgical resection is reported to be good, a variable prognosis has been reported. The size of the tumor, histological type, nodal involvement, and distant metastasis are thought to affect the prognosis. Herein we present an elderly patient with chest wall hamartoma and typical carcinoid, in the light of literature.Introduction
The term "hamartoma" originates from the Greek word "hamartanein," meaning "to go wrong," and was first defined by Albrecht in 1904 as the mislocalization of tissues normally found in an organ. Hart reported hamartoma localized in the lungs for the first time in 1906. Hamartoma is the most common benign tumor of the lung [1,2]. Although it can occur in any organ, such as the lung, kidney, liver, and hypothalamus, domestic and foreign literature reports on chest wall hamartoma mainly focus on infants, but hamartoma on the adult chest wall is extremely rare, and the number of reported cases is limited [3]. The incidence of typical carcinoid tumor has decreased in recent years. In this case report, we aimed to present an elderly patient with chest wall hamartoma and typical carcinoid coexistence.Case Presentation
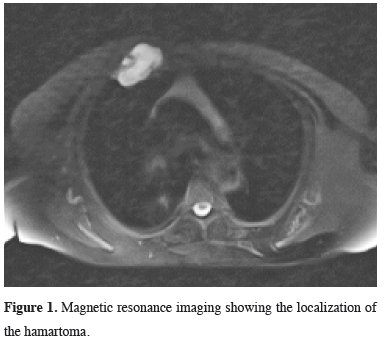
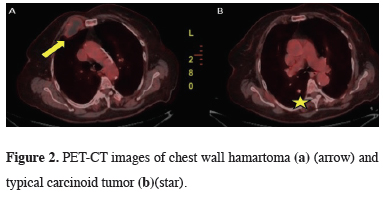
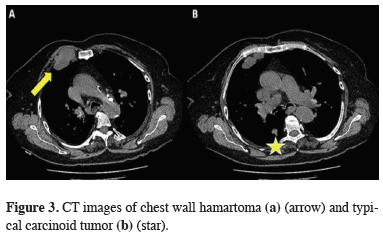
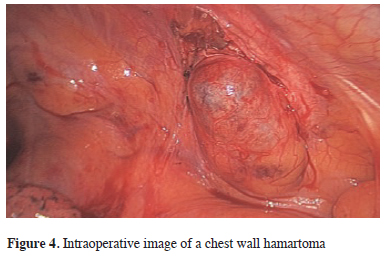
An 84-year-old female patient with no known diseases other than hypertension and diabetes mellitus. She presented with swelling and pain on the anterior chest wall at the right edge of the sternum. Physical examination revealed a swelling in the right parasternal area that was painful to touch. Magnetic Resonance Imaging (MRI) was examined (Figure 1). Positron Emission Tomography (PET-CT) was planned for the patient upon the interpretation that there was an anteriorly subcutaneous expansile multilobulated mass lesion approximately 50×38×57 mm in size, destructing the 3rd costa in the right parasternal area. The PET-CT report was interpreted as an irregular, limited lesion (SUVMax = 2.22) on the right hemithorax anterior chest wall in the lateral neighborhood of the sternum and a spicular lesion (SUVMax = 2.37) in the posterior upper lobe of the right lung, and an operation plan was made for the patient (Figures 2,3). A video-assisted right thoracotomy was performed due to the patient’s pulmonary function test showed FEV1 best: 0.96, low respiratory capacity, and one of the lesions was located in the chest wall and the other in the parenchyma. A wedge resection was performed on the lesion located in the upper lobe of the right lung, and the frozen section was sent for examination. The frozen section result was reported as malignant. Anatomic resection could not be performed because the patient had limited respiratory reserve. The lesion adjacent to the inferior mamamarian artery and sternum was identified. (Figure 4). The mass on the chest wall was removed by blunt and sharp dissections and sent to pathology. No early complications were observed. In pathological examination, the wedge resection material from the upper lobe was reported as a 1.8×7.5 cm typical carcinoid tumor, and the material removed from the chest wall was reported as 4.5×3.5×1 cm compatible with hamartoma (Figure 5). The patient is being followed up by oncology due to the typical carcinoid diagnosis. Consent was obtained from the patient for the use of her medical data in academic studies.){kind=link}
){kind=link}
){kind=link}
){kind=link}
){kind=link}
 Click Here to Zoom |
Figure 1: Magnetic resonance imaging showing the localization of the hamartoma. |
 Click Here to Zoom |
Figure 2: PET-CT images of chest wall hamartoma (a) (arrow) and typical carcinoid tumor (b)(star). |
 Click Here to Zoom |
Figure 3: CT images of chest wall hamartoma (a) (arrow) and typical carcinoid tumor (b) (star). |
 Click Here to Zoom |
Figure 4: Intraoperative image of a chest wall hamartoma |
 Click Here to Zoom |
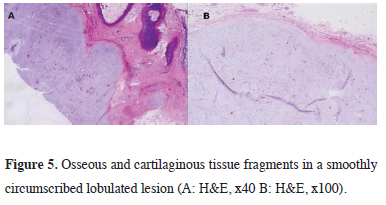
Figure 5: Osseous and cartilaginous tissue fragments in a smoothly circumscribed lobulated lesion (A: H&E, x40 B: H&E, x100). |
Discussion
Hamartoma means an abnormal combination of normal tissue elements or an abnormal ratio of a single element in an organ, and is the most common benign tumor of the lung. However, hamartomas arising from the chest wall are quite rare and present with deformity of the thoracic wall and respiratory symptoms in varying degrees at birth or early infancy [4]. In this case, in contrast to the literature, the patient was advanced aged and had coexistence with typical carcinoid tumor. Neuroendocrine tumors (NETs) are a subtype of neoplasms that can arise in most organs and share several common biochemical and pathological features. Pulmonary NETs account for 20-30% of all NETs, and NETs in the lung can be divided into four subtypes according to their degree of malignancy: Typical carcinoids (TC), atypical carcinoids (AC), large cell neuroendocrine carcinomas (LCNEC), and small cell lung cancers (SCLC). Among these subtypes, typical and atypical carcinoids are generally referred to as pulmonary carcinoids and constitute 1-2% of all pulmonary malignancies; however, their incidence has increased markedly in recent years [5]. Since pulmonary carcinoid is a tumor with a low malignancy rate, resection is usually an effective treatment option for early disease. However, in this case, anatomical resection could not be performed because of insufficient respiratory reserve. Approximately 80% of pulmonary carcinoids are located in the central airways [6], whereas the number of reported cases of chest wall hamartomas in adults is very low [3]. To the best of our knowledge, no case of coexistence of chest wall hamartoma and typical carcinoma has been reported in the literature. During the treatment period, MRI and PET-CT imaging techniques were used to examine the detailed localization of the lesions, their metabolic activity, and their relationship with soft tissue and parenchyma. Since our preoperative FEV 1 best: 0.96, our operation plan was made in such a way that both lesions could be reached through a single incision line and video-assisted, although both lesions were distant from each other and in different localizations. Although frozen section examination was reported as a typical carcinoid tumor, anatomical resection could not be performed due to the insufficient respiratory reserve.In conclusion, hamartomas of the chest wall at an advanced age are very rarely reported pathologies and require detailed preoperative examination and differential diagnosis. They may coexist with other pathologies, such as the typical carcinoid that we found in our patient, and surgery is the most effective treatment method.
Declaration of Conflicting Interests
The authors declared no conflicts of interest with respect
to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Authors’ Contributions
RY,MSO: data curation, investigation, methodology,
validation, writing, review and editing, SEA,HEC: conceptualization,
data curation, resources, supervision,
writing, review and editing, OA: data curation, investigation.
Reference
1) Mertoğlu A, Eroğlu A, Kürkçüoğlu C, Karaoğlanoğlu N, Polat
P, Balcı AE. İnisyal bronkoskopik tedavi uygulanan tipik karsinoid
tümör olgusu. Turk Gogus Kalp Damar Cerrahisi Derg
2011; 19: 121-4.
2) Crouch JD, Gabriele OF, Stevens CW, Welsh RJ. A clinical
review of patients undergoing resection for pulmonary hamartoma.
Am Surg 1988; 54: 297-9.
3) Ahmed S, Singla A, Thakur N, Sharma D, Bajaj Y, Ranga R. A
rare case of laryngeal hamartoma. Indian J Otolaryngol Head
Neck Surg 2021; 73: 1-3.
4) Önen A, Yüksel M, Toker A, Tanju S, Kuzucu A, Demirkaya
A. Pulmonary hamartoma and squamous cell carcinoma: a
very rare coexistence. Turk Gogus Kalp Damar Cerrahisi Derg
2007; 15: 311-3.