


2Department of Radiology, Lahore Medical and Dental College, Lahore, Pakistan DOI : 10.26663/cts.2025.031
Summary
Fibro-osseous lesions of the rib are rare benign entities that frequently mimic primary or secondary chest wall malignancies. They are most commonly reported in the sixth to eighth ribs, with lower rib involvement being exceptionally uncommon. Radiological findings are often nonspecific, thus, histopathological evaluation is crucial for establishing a definitive diagnosis. We report the case of a 32-year-old female presenting with left lower chest pain and a firm, gradually expanding swelling over the left posterolateral chest wall. Imaging revealed a lytic lesion of the left 11th rib, raising suspicion of a primary bone tumor. Given the diagnostic uncertainty, resection of the affected rib segment was performed. The postoperative course was uneventful, and the patient was discharged on the fourth postoperative day. Histopathology confirmed a benign fibro-osseous lesion. Fibro-osseous lesions of the rib are rare and diagnostically challenging due to their radiological resemblance to malignant tumors. Involvement of the 11th rib is infrequent, and to our knowledge, has not been previously documented. This case showed the importance of surgical excision in achieving diagnostic certainty in the case of a fibro-osseous lesion.Introduction
Fibro-osseous lesions of the rib are exceptionally rare, benign tumors that often resemble malignant or aggressive chest wall neoplasms on clinical and radiological evaluation. These tumors are also labelled as post-traumatic fibro-osseous lesions (PTFOL), and regarded as reactive proliferations arising after minor or unrecognized trauma, and have historically been misdiagnosed as rib metastases, osteoid osteomas, fibrous dysplasias, sclerosing xanthomatous lesion, or benign fibrous histiocytomas [1-3]. The sixth to eighth ribs are most frequently involved, with no consensus on their natural history or optimal management [4]. The clinical challenge lies in their radiological resemblance to primary or secondary chest wall malignancies. Histopathological confirmation remains the gold standard for diagnosis, as imaging alone rarely provides sufficient specificity [5].Case Presentation
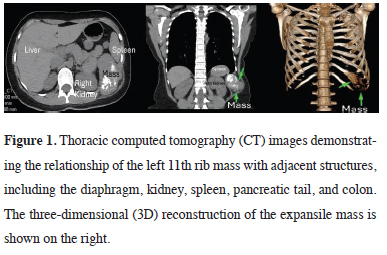
A 32-year-old female with a six-month history of dull left chest wall pain had a firm, non-tender swelling over the 11th rib. Computed tomography (CT) showed a well-circumscribed, expansile mass (90 × 78 × 50 mm) with arc-like calcification involving the anterior 11th rib and projecting into the abdominal cavity, without invasion or metastasis (Figure 1). A tru-cut biopsy suggested a spindle cell neoplasm.){kind=link}
 Click Here to Zoom |
Figure 1: Thoracic computed tomography (CT) images demonstrating the relationship of the left 11th rib mass with adjacent structures, including the diaphragm, kidney, spleen, pancreatic tail, and colon. The three-dimensional (3D) reconstruction of the expansile mass is shown on the right. |
Due to the diagnostic uncertainty and symptomatic presentation, she underwent wide local resection of the 10th and 11th ribs with 2 cm margins, followed by chest wall reconstruction using polypropylene mesh. The postoperative recovery was uneventful, and the patient was discharged on the fourth postoperative day.
Histopathological examination revealed a well-circumscribed, lobulated rib mass (7.8 × 7 × 4 cm) with a homogeneous tan-white cut surface. Microscopically, curvilinear osteoid trabeculae lined by osteoblasts were seen, with spindle cell proliferation showing minimal atypia and mild stromal fibrosis. No high-grade features, necrosis, or significant mitotic activity were observed. Immunohistochemistry: CD34, Desmin, STAT6, MUC4 negative; SATB2 positive; β-catenin cytoplasmic only. Final diagnosis was fibro-osseous lesion with clear resection margins (Figure 2). At nine months, the patient remained asymptomatic and recurrence-free. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
){kind=link}
Discussion
Fibro-osseous lesions of the ribs are exceedingly rare, leading to diagnostic and therapeutic challenges. In this patient, a mass involving the left 11th rib, projecting into the abdominal cavity, initially raised strong suspicion for a primary malignant chest wall tumor. The pre-operative tru-cut biopsy further reinforced the malignant differential, necessitating surgical resection. However, final histopathology confirmed a benign fibro-osseous lesion.The reported age range of post-traumatic fibro-osseous lesions (PTFOL) varies widely, from adolescence to late adulthood, with a mean age in the fifth decade of life [3,4]. Our patient, a 32-year-old female, represents the younger spectrum of reported cases. While a history of trauma has been suggested as a precipitating factor in the majority of PTFOL cases [3], our patient denied any prior traumatic episode. This observation supports the hypothesis that such lesions may also arise in the absence of overt trauma, potentially representing a reactive or developmental process [6].
Radiologically, fibro-osseous rib lesions typically present as well-circumscribed, expansile masses with varying internal density and occasional calcification [1,3]. In our case, CT imaging revealed a large mass with arc-like calcifications and an expansile pattern, raising suspicion for a malignant chest wall tumor. Such radiological overlap complicates the preoperative diagnostic process. A structured diagnostic approach is therefore essential, including initial imaging (CT or MRI), core needle biopsy, and immunohistochemistry (β-catenin, SATB2) to distinguish fibro-osseous lesions from mimickers such as fibrous dysplasia or low-grade sarcomas [7,8]. Definitive histopathology following excision is crucial, particularly in large or symptomatic lesions.
Histopathological examination remains the gold standard for diagnosis. In our case, the initial biopsy yielded a spindle cell neoplasm, which was misleading, and the correct diagnosis was only possible after complete excision and thorough histological evaluation. Fibrous dysplasia and osteoid osteoma are the most common benign rib lesions and can be distinguished from fibro-osseous lesions histologically [3,4]. The absence of nuclear β-catenin staining and positivity for SATB2 further supported the fibro-osseous nature of the lesion in our patient.
Surgical management remains the mainstay for rib tumors when malignancy cannot be excluded preoperatively. A wide local resection of the involved ribs with mesh reconstruction was performed in our patient, with good functional outcome. While some small, asymptomatic fibro-osseous lesions confirmed by biopsy may be managed conservatively [1,5], surgery is warranted in cases with diagnostic uncertainty, symptomatic lesions, or large tumors threatening adjacent structures.
Importantly, long-term outcomes remain poorly defined. Recurrence has not been systematically reported due to the rarity of these lesions and limited follow-up in existing studies [2,4]. Our 9-month disease-free followup, although reassuring, does not allow conclusions about long-term prognosis. Extended surveillance is therefore recommended to clarify recurrence risk and natural history.
In conclusion, fibro-osseous lesions of the rib are rare entities that can closely mimic malignant chest wall tumors. This case highlights the importance of maintaining PTFOL in the differential diagnosis of rib masses, especially when imaging suggests malignancy. A structured diagnostic framework combining radiology, biopsy, and immunohistochemistry is essential, but complete surgical resection remains the definitive management strategy in cases of diagnostic uncertainty (Figure 3). Future multicenter registries could help clarify the natural history and optimal surveillance strategies for these lesions.
){kind=link}
Figure 3. Diagnostic workflow for the evaluation of rib masses suspicious for fibro-osseous lesions.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect
to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Authors’ contribution
MSN: Conceptualization, Methodology, Supervision,
Writing – review & editing. ZS: Writing – original draft,
Visualization, Data curation. KF: Investigation, Validation
(Radiology).
Reference
1) Nassereddine H, Larousserie F, Campagna R, Castier Y, Couvelard
A, Choudat L et al. Xanthomatous posttraumatic fibroosseous
lesion of the rib: a rare and underrecognized entity. Case
report and literature review. Int J Surg Pathol 2017; 25: 640-3.
2) Blanco M, Cabello-Inchausti B, Cura M, Fernandes L. Posttraumatic
fibro-osseous lesion of the ribs and scapula (sclerosing
xanthofibroma). Ann Diagn Pathol 2001; 5: 343-9.
3) McDermott MB, Kyriakos M, Flanagan FL. Posttraumatic fibro-
osseous lesion of rib. Hum Pathol 1999; 30: 770-80.
4) Aubert S, Kerdraon O, Conti M, Buob D, Petit S, Leroy X.
Post-traumatic fibro-osseous lesion of the ribs: a relatively under-
recognised entity. J Clin Pathol 2006; 59: 635-8.
5) Brahem M, Jomaa O, Abdelali M, Sarraj R, Bayoudh A, Njim L
et al. Post-traumatic fibro-osseous lesion of the fourth rib simulating
a chest wall tumor: a case report. Korean J Fam Med
2023; 44: 295-8.
6) Patel R, Parelkar K, Puthenpurayil S, Kothiya MR. Cementoossifying
fibroma: an extensive fibro-osseous lesion involving
paranasal sinuses. Int J Otorhinolaryngol Head Neck Surg
2024; 10: 595-8.