



Summary
Poland’s syndrome is a rare developmental anomaly characterized by absence of pectoralis major muscle and presence of ipsilateral hand abnormalities (mostly syndactyly). Numerous malformations as a component of this syndrome was defined in literature such as congenital heart diseases, upper limb anomalies and pulmonary or renal hypoplasia. The incidence of Poland’s syndrome ranges from 1 in 7,000 to 1 in 100,000 live births. Here we describe a rare case of patient with Poland’s syndrome with contralateral spontaneous pneumothorax.Introduction
Although various abnormalities were defined as a component of Poland’s syndrome in the literature, the characteristic features of this syndrome are absence of pectoralis major muscle and presence of ipsilateral hand abnormalities. Poland’s anomaly with ipsilateral pneumothorax has been reported before as a very rare coexistence, but contralateral occurrence of pneumothorax is an extraordinary clinical situation and this case would be an important example of bilateral effect of Poland’s syndrome on the lung parenchyma.Case Presentation
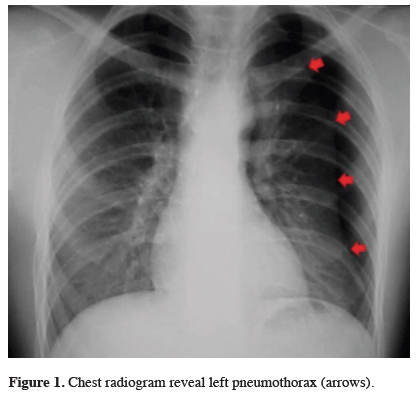
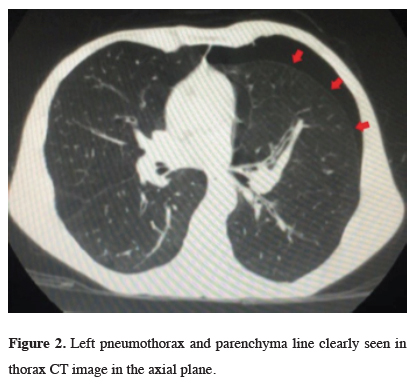
58-years-old male admitted our emergency department with left chest pain, cough and shortness of breath. He was afebrile with a heart rate of 115/min, blood pressure of 125/75 mmHg, respiratory rate of 25/min and oxygen saturation of 80% on room air. His medical and family history was unremarkable. His social history revealed 10 pack-year cigarette smoking. The physical examination revealed a middle aged, dyspneic male, with an asymmetric chest wall due to hypoplasia of his right pectoral muscle and syndactyly in his right hand. His breathing sounds on auscultation were decreased over the left lung field. These clinical findings and chest radiogram (Figure 1) revealed Poland’s anomaly with left sided pneumothorax. After the patient’s clinical condition stabilized, hand radiography and thorax computed tomography were obtained (Figure 2).){kind=link}
){kind=link}
 Click Here to Zoom |
Figure 1: Chest radiogram reveal left pneumothorax (arrows). |
 Click Here to Zoom |
Figure 2: Left pneumothorax and parenchyma line clearly seen in thorax CT image in the axial plane. |
 Click Here to Zoom |
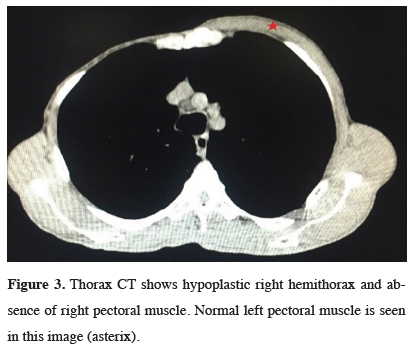
Figure 3: Thorax CT shows hypoplastic right hemithorax and absence of right pectoral muscle. Normal left pectoral muscle is seen in this image (asterix). |
 Click Here to Zoom |
Figure 4: One of the clinical component of Poland’s syndrome: hand abnormalities (absence of medial phalanges in right hand) Normal left medial phalanges are seen in this image (asterix). |
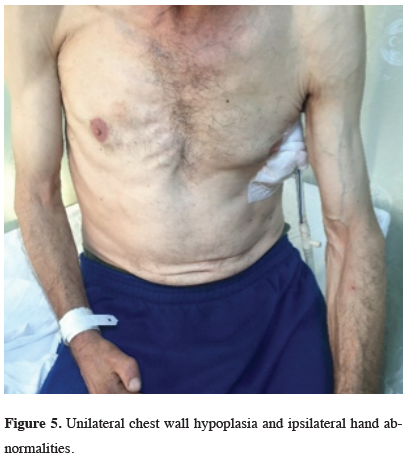
Tube thoracostomy was performed from the fifth intercostal space on midaxillary line (Figure 5). His symptoms relieved after the intrapleural air was evacuated.
){kind=link}
 Click Here to Zoom |
Figure 5: Unilateral chest wall hypoplasia and ipsilateral hand abnormalities. |
Lung expansion was obtained on 4th day of drainage. Chest tube was removed and patient was discharged at 5th day of hospitalization.
Discussion
Alfred Poland described Poland’s syndrome in 1841. Although chest wall hypoplasia and hand abnormalities were defined as the characteristic features of this syndrome, many other musculoskeletal anomalies would be seen like agenesis of the ribs and sternum, scoliosis, brachysyndactyly, mammary aplasia, and absence of the latissimus dorsi and serratus anterior muscles [1-3].In literature, there are few reports about the familial occurrence of Poland’s syndrome but, it was thought to be an intrauterine pathology rather than a genetic defect [4]. The etiology is unknown but hypoxia during in the sixth to seventh week of gestation is thought to be a main etiological factor causing hypoplastic or aplastic musculoskeletal abnormalities. The possible cause of the hypoxia would be arterial spasm or an arterial malformation [4,5].
Poland’s anomaly with spontaneous pneumothorax has been previously reported only in few cases [6,7]. We detected only one case Poland’s anomaly with contralateral spontaneous pneumothorax.
In literature, emphysema has been shown to be associated with spontaneous pneumothorax and it is defined as an “abnormal permanent enlargement of air spaces distal to the terminal bronchioles”. Main pathology is the destruction of lung’s epithelial barrier causing a decrease in pulmonary elastic recoil. Cigarette smoke exposure is generally the main activator of destruction cascade. In addition, hypoxia would aggravate oxidative stress and protease production resulting emphysematous changes in the lung.
Considering the pathophysiology of Poland’s syndrome based on hypoxia, etiological factors that cause this syndrome may also be responsible for the occurrence of bulla formation and emphysematous changes in lung. In addition, different brachial arch blood supply defects might be responsible for the contralateral occurrence of pneumothorax [7].
Consequently a little is known about the relationship between pathogenesis of Poland’s syndrome and pneumothorax. More such should be presented to identify the relationship of these two diseases.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Reference
1) Forkin AA, Robisec F. Poland’s syndrome revisited. Ann Thorac Surg 2002; 74: 2218-25.
2) Bouvet JP, Leveque D, Bernetieres F, Gros JJ. Bouvet JP. Vascular origin of Poland syndrome? A comparative rheographic study of the vascularisation of the arms in eight patients. Eur J Pediatr 1978; 128: 17-26.
3) Wilson MR, Louis DS, Stevenson TR. Poland’s syndrome: variable expression and associated anomalies. J Hand Surg Am 1988; 13: 880-2.
4) Sujansky E, Riccardi VM, Matthew AL. The familial occurrence of Poland syndrome. Birth Defects Orig Artic Ser 1977; 13: 117-21.
5) Beer GM, Kompatscher P, Hergan K. Poland’s syndrome and vascular malformations. Br J Plast Surg 1996; 49: 482-4.