



2Department of Thoracic Surgery, Cigli Regional Training Hospital, Izmir, Turkiye DOI : 10.26663/cts.2020.00016
Summary
Background: The most common injury associated with blunt thoracic trauma is the rib fracture. Outpatients, who had a minor blunt trauma that did not form any complications, present more than half of the rib fractures. Unfortunately, there are several limitations on the chest x-ray. In this study, we investigated the efficacy of ultrasonography in the diagnosis of rib fractures resulting from blunt thoracic trauma.Materials and Methods: Fifty-eight patients who were admitted to the Thoracic Surgery Outpatient Clinic in our center due to minor thoracic trauma between October 2017 and July 2018 were included in the study. All patients underwent chest radiography, and thorax US after a detailed history and physical examination were performed.
Results: Of the 58 patients included in the study, 33 (56.9%) were male, and 25 (43.1%) were female, while the mean age was 46.79 ± 15.75 years. While the rib fractures were detected in 24 patients with chest x-ray, US detected rib fractures in 47 patients. The comparison between the two examinations, the superiority of the US in the diagnosis of rib fracture was statistically significant compared to the chest radiography (p < 0,001).
Conclusions: We believe that preferring ultrasound instead of thorax CT for its less radiation and lower cost at the next step beyond chest x-ray for patients, who applied to the outpatient clinic with minor trauma and whose general condition is well, is more beneficial.
Introduction
The most common injury associated with blunt thoracic trauma is the rib fracture [1,2]. More than half of rib fractures are presented by outpatients who had a minor blunt trauma that did not form any complications [3]. Rib fractures are clinically suspected in the presence of the related history of the patient, coughing, and localization of the pain with palpation and deep breathing [2]. Unfortunately, there are several limitations on the chest x-ray [4,5]. Costal cartilage fractures could be radiologically overlooked unless the densely calcified cartilage is broken [4]. Besides, obesity and co-existing lung conditions may adversely affect the quality of the radiography and may cause difficulty in interpreting and diagnosing the image [6]. Due to the adjacency of abdominal soft tissues in the lower rib fractures, it is difficult to interpret the radiograph [5]. Accurate identification of rib fractures with ultrasonography (US) in the presence of clinical suspicion usually does not significantly change the patient management, but in fact, leads to significant advantages in practice [7].In this study, the efficacy of ultrasonography in the diagnosis of rib fractures resulting from blunt thoracic trauma was investigated.
Methods
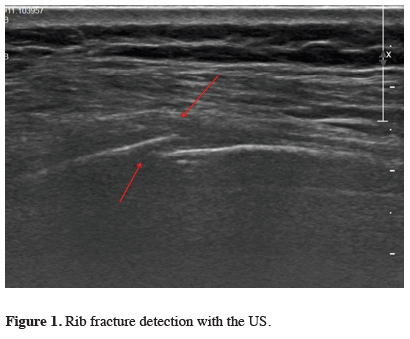
Following institutional review board approval (1204/2019), fifty-eight patients who were admitted to the Thoracic Surgery Outpatient Clinic in our center due to minor thoracic trauma between October 2017 and July 2018 were included in the study. Minor traumas were evaluated as traumas there may be rib fractures without pneumothorax, hemothorax, or pulmonary contusion. All patients underwent chest radiography, and thorax US after a detailed history and physical examination were performed. An experienced radiologist performed the chest x-ray evaluation and ultrasonography, and a thoracic surgeon performed the clinical evaluation. Ultrasonography was performed on the same day after chest x-ray.The chest x-ray (Samsung, GC80, Korea) was performed without a grid nearly 180 cm in posterioanterior position with a 85 kVp and 3.2 mAs. Ultrasonography was performed on patients by the radiologist using a 5-12 MHz linear array probe. Ultrasonography was performed longitudinally in such a way that the patient was in a lying or sitting position, starting from the place where the physical examination was most painful, including the adjacent ribs. During the ultrasound examination, cortical border irregularity, acoustic edge shadow, and local hematoma criteria were taken into consideration (Figure 1). Ultrasonography and chest radiography results were compared.
){kind=link}
 Click Here to Zoom |
Figure 1: Rib fracture detection with the US. |
Statistical Analysis
Data were analyzed retrospectively. The variables were reported as mean and standard deviation (SD) with a confidence interval (CI) of 95%. Mean values were compared with the Student’s T-test and one-way analysis of variance (ANOVA). The ratios of categorical variables were given in percentages and compared with Fisher’s Exact test or Pearson’s chi-square test. In addition, sensitivity and specificity values are given as a result. The significance level was accepted as p < 0.05. All analyses were performed using SPSS 22.0 (SPSS Inc. Chicago, Illinois, USA) software.
Results
Of the 58 patients included in the study, 33 (56.9%) were male, and 25 (43.1%) were female, while the mean age was 46.8 ± 15.8 years. The reason for the reference to the outpatient clinic was falling for 49 patients (84.5%), traffic accidents for five patients (8.6%), and assault was four patients (6.9%). The patients were admitted to the outpatient clinic with an average of 4.3 (1-20) days after the trauma, while the application was on the 3rd day most frequently. The mean duration of the ultrasound examination was 10.36 ± 0.325 minutes. 31 patients had right-sided (53.5%), 26 patients had left-sided (44.8%) and one patient had bilateral (1.7%) pain (Table 1). The total number of fractures detected by chest x-ray was 37, and the total number of fractures detected by the US was 94.){kind=link}
Table 1: Characteristics of the study group.
While the rib fractures were detected in 24 patients with chest x-ray, US detected rib fractures in 47 patients. The total number of fractures detected by chest x-ray was 37, and the total number of fractures detected by the US was 94. As a result of the comparison between the two examinations, the superiority of the US in the diagnosis of rib fracture was statistically significant compared to the chest radiography (p < 0,001) (Table 2).
){kind=link}
Table 2: Detection of the rib fracture.
In the rib fracture diagnosis, the sensitivity of chest x-ray and US were 48.9% and 97.9%; specificity was 90.9% and 90.9%; positive predictive value (PPV) was 95.8% and 97.9%; negative predictive value (NPV) 29.4% and 90.9%; the accuracy rate was 56.9% and 96.6%, respectively (Table 3).
){kind=link}
Discussion
The rib fractures are the most common thoracic injury. Fractures exist in only 32 - 42% of symptomatic patients [2,8]. The main symptom of rib fracture is the pain in the area of movement or the non-moving injury area [9]. Physical examination and chest x-ray are the initial diagnostic methods for the detection of rib fractures and are the main diagnostic tools [1,5]. The presence of crepitation in the physical examination may lead to the diagnosis, but this may not be the case for minor traumas. There are also several limitations in plain chest radiography [5]. In these patients, only 49% of rib fractures were detected by a precise physical evaluation and chest x-ray [1]. Obesity and co-existing lung disorders may adversely affect the quality of radiography, which is a challenge to interpret and diagnose the image [6]. Besides, some patients may not provide a suitable position during the plain radiography procedure and may cause limitations in the radiological examination [8]. Rib fractures could be detected in 50-80% of patients with minor chest trauma by conventional radiological examination for various reasons [8].Ultrasound examination has become popular in recent years as a useful and non-invasive diagnostic tool [5]. There are studies in which ultrasonography has better results than chest x-ray in the diagnosis of rib fractures [4,6,10,11]. In a meta-analysis, the specificity and sensitivity of the US were reported to be better [12]. Studies are reporting that ultrasound is also useful in sternal fractures [13,14]. Chan reported that the US has higher accuracy in thoracic bone fractures [7]. The sensitivity, specificity, and efficacy values of ultrasound in the diagnosis of rib fracture were found to be better than chest radiography in our study in accordance with the literature. Our patients were admitted to the outpatient clinic an average of 4.3 days after trauma. Hwang et al reported that no significant effect on the results that duration time until the US examination [5].
Being non-invasive, portable, relatively inexpensive, non-radiation and reproducible are the most critical advantages of ultrasonography and these make ultrasonography a valuable diagnostic tool [1]. It is also a reliable diagnostic tool for pregnant patients [8]. A plain chest x-ray may overlook uncalcified rib fractures, especially in costal cartilages [3]. It is known that ultrasound is more sensitive than plain x-ray and tomography in such fractures [8]. Studies are showing that ultrasound could better detect costal cartilage fractures and costochondral junction fractures [4,10]. Griffith et al [10] reported that plain chest radiography could detect rib fractures in 12% of patients with chest trauma, while ultrasonography could detect in 78% and ultrasonography was more sensitive. In our study, rib fracture was detected in 41.4% of patients with chest x-ray and 81% with the US. Martino et al [15] argued that ultrasonography is more useful in rib and costal cartilage fractures and should be performed in every patient with chest trauma as it could detect internal organ injuries.
Accurate identification of rib fractures by ultrasonography in case of clinical suspicion usually provides some advantages in practice, although it does not substantially alter patient management. First, with the early diagnosis of rib fractures, it might be necessary to initiate an appropriate pain management protocol that confirms the use of analgesic therapy or intercostal nerve blockages. Medical advice on employee return to work and activities is essential [7]. Meanwhile, the US is an easy, accessible, rapid, and accurate diagnostic procedure in hemodynamically unstable patients with hemothorax and/or pneumothorax [1]. The diagnosis of rib fracture is also important in terms of the medico-legal perspective [2,16]. The significant ultrasonography disadvantages are the difficulty in diagnosis in large-breasted patients, obesity, fractures in the ribs under the scapula, or the first rib fractures below the clavicle [1,5,8].
In conclusion, we believe that preferring ultrasound instead of thorax CT for its less radiation and lower cost at the next step beyond chest x-ray for patients, who applied to the outpatient clinic with minor trauma and whose general condition is well, is more beneficial. With more studies including more centers and the number of patients, ultrasonography would be used more widely as a result of supporting the effectiveness of ultrasonography in the diagnosis of rib fracture.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support for the research and/or authorship of this article.
Reference
1) Psihbin E, Ahmadi K, Foogardi M, Salehi M, Seilanian Toosi F, Rahimi-Movaghar V. Comparison of ultrasonography and radiography in diagnosis of rib fractures. Chin J Traumatol 2017;20:226-8.
2) Hurley ME, Keye GD, Hamilton S. Is ultrasound really helpful in the detection of rib fractures? Injury 2004;35:562-6.
3) Turk F, Kurt AB, Saglam S. Evaluation by ultrasound of traumatic rib fractures missed by radiography. Emerg Radiol 2010;17:473-7.
4) Malghem J, Vande Berg B, Lecouvet F, Maldaque B. Costal cartilage fractures as revealed on CT and sonography. AJR Am J Roentgenol 2001;176:429-32.
5) Hwang EG, Lee Y. Simple X-ray versus ultrasonography examination in blunt chest trauma: Effective tools of accurate diagnosis and considerations for rib fractures. J Exerc Rehabil 2016;12:637-41.
6) Kara M, Dikmen E, Erdal HH, Simsir I, Kara SA. Disclosure of unnoticed rib fractures with the use of ultrasonography in minör blunt chest trauma. Eur J Cardiothorac Surg 2003;24:608-13.
7) Chan SS. Emergency bedside ultrasound for the diagnosis of rib fractures. Am J Emerg Med 2009;27:617-20.
8) Lee WS, Kim YH, Chee HK, Lee SA. Ultrasonographic evaluation of costal cartilage fractures unnoticed by the conventional radiographic study and multidetector computed tomography. Eur J Trauma Emerg Surg 2012;38:37-42.
9) Mayberry JC, Trunkey DD. The fractured rib in chest Wall trauma. Chest Surg Clin N Am 1997;7:239-61.
10) Griffith JF, Rainer TH, Ching AS, Law KL, Cocks RA, Metreweli C. Sonography compared with radiography in revealing acute rib fracture. AJR Am J Roentgenol 1999;173:1603-9.
11) Rainer TH, Griffith JF, Lam E, Lam PK, Metreweli C. Comparison of thoracic ultrasound, clinical acumen, and radiography in patients with minör chest injury. J Trauma 2004;56:1211-3.
12) Yousefifard M, Baikpour M, Ghelichkani P, Asady H, Darafarin A, Esfahani MRA et al. Comparison of ultrasonography and radiography in detection of thoracic bone fractures; a systematic review and meta-analysis. Emergency 2016;4:55-64.
13) Hendrich C, Finkweitz U, Berner W. Diagnostic value of ultrasonography and conventional radiography fort he assessment of sternal fractures. Injury 1995;26:601-4.
14) Jin W, Yang DM, Kim HC, Ryu KN. Daignostic values of sonography for assessment of sternal fractures compared with conventional radiography and bone scans. J Ultrasound Med 2006;25:1263-8.