



2Department of Thoracic Surgery, Sanliurfa Medical Practice and Research Center, Sanliurfa, Turkey
3Department of Pathology, University of Health Sciences, Dr Suat Seren Chest Diseases and Surgery Medical Practice and Research Center, İzmir, Turkey DOI : 10.26663/cts.2021.0007
Summary
Tuberculosis and bronchiectasis are the most common causes of the destroyed lung. Mediastinal masses, which cause bronchial compression, can also cause bronchiectasis. Chronic lymphocytic leukemia (CLL) is the most common subtype of leukemia, and it can rarely cause bronchiectasis and destroyed lungs by causing a mass effect in the mediastinum. A 50-year-old female patient with a history of tuberculosis in her childhood admitted to our clinic with dyspnea, cough, and chest pain. During the clinical examinations, a solid mass with approximately 46x33 mm in size was observed in the posterior mediastinum, compressing the left main bronchus and the entire left lung was destroyed. Since the patient had no definite diagnosis and was symptomatic, a surgical treatment was planned, and left pneumonectomy was performed together with mediastinal mass excision. As a result of the extracted specimen histopathology, bronchiectasis was present, and the mediastinal mass was consistent with chronic lymphocytic leukemia. The patient did not experience any postoperative complications and was referred to the oncology clinic for follow-up and treatment. Herein, we aimed to present a case with chronic lymphocytic leukemia mass in the posterior mediastinum compressing the left main bronchus, which caused bronchiectasis and destroyed lung with the literature’s accompaniment.Introduction
The term “destroyed lung” is used for widespread lung injury caused by pulmonary infectious diseases [1]. The most common causes are bronchiectasis and tuberculosis [2]. Chronic lymphocytic leukemia (CLL) is a disease that occurs with the increase of mature lymphocytes without proliferation in the spleen, blood, bone marrow, lymph nodes. Thoracic symptoms of CLL can be classified as leukemia or treatment-related immunodeficiency, pleural effusions, and specific bronchopulmonary involvement because of lymphocytic infiltration. It is rare for CLL to cause bronchial compression due to the mass effect.Accompanied by the literature, we aimed to present a destroyed lung case caused by CLL’s mass effect in the posterior mediastinum, since it is infrequent.
Case Presentation
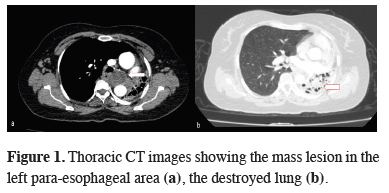
A 50-year-old female patient was applied to another hospital 5 years ago due to screening for a job admission and a mediastinal mass was detected in computed tomography. In this center, a transbronchial biopsy was performed. However, a definitive diagnosis could not be done. At that time the patient applied to our clinic, and in the computed tomography report a 2x1.7 cm soft tissue lesion in the left paraesophageal area was detected. Hospitalization was recommended for further examination and treatment, but the patient refused, as she had no symptoms and discontinued her follow-ups.The second application of the patient to our clinic was 5 years later with complaints of shortness of breath, cough and chest pain. In her anamnesis, she had a history of tuberculosis during the childhood period. At the physical examination, respiratory sounds could not be detected on the left hemithorax and there was no palpable lymphadenopathy at any other part of the body. The sedimentation rate was 25mm/h. The other laboratory parameters were in normal ranges except mild leukocytosis. There was no growth in the tuberculosis culture of the bronchial sample taken from the patient. Abdominal ultrasonography was normal. Computed tomography of the thorax revealed a well-circumscribed, 46x33 mm mass lesion in the left para-esophageal area, springing the descending aorta to the left and compressing the left main bronchus. The left lung was destroyed, mediastinal shift was apparent together with the hyperaeration of the right lung (Figure 1).
){kind=link}
 Click Here to Zoom |
Figure 1: Thoracic CT images showing the mass lesion in the left para-esophageal area (a), the destroyed lung (b). |
During the fiberoptic bronchoscopy, a long segment external compression was detected starting from the trachea’s distal level descending to the left main bronchus. Diffuse edema and abundant mucopurulent secretion was present in the left main bronchus. Pseudomonas aeroginosa was reproduced in the culture. Antibiotic treatment of piperacilin-tazobactam in compliance with the culture taken was initiated. Respiratory function test results were as follows; FEV1: 1.07 (51%), FVCex: 1.57 (57%), FEV1/FVC: 76% (96%). According to lung ventilation-perfusion scintigraphy results, no functional lung tissue was reported in the left lung area and the patient was appropriate for left a pneumonectomy. With the present findings, an operation was planned for both the diagnosis and treatment. Mediastinal mass excision and pneumonectomy was performed via left thoracotomy. The patient, was discharged on the 5th postoperative day without any complications. The histopathological diagnosis was bronchiectasis, and the mediastinal mass was compatible with chronic lymphocytic leukemia (Figure 2). The patient was referred to the oncology clinic for further treatment.
){kind=link}
 Click Here to Zoom |
Figure 2: Excised material of the mass lesion (a), pneumonectomy specimen (b) and histopathological view of small 129 atypical lymphoid cells (H&E; x1000) (c). |
Written informed consent was obtained from the patient for publication of her data.
Discussion
Tuberculosis comes first among the causes of the destroyed lung, followed by chronic pulmonary infections such as bronchiectasis, chronic interstitial pneumonia, organizing pneumonia, and aspergillosis [3]. Pneumonectomy is necessary due to complications such as massive hemoptysis caused by destroyed lung, secondary fungal infections, secondary amyloidosis, or pulmonary-systemic shunt [4]. There was a history of tuberculosis in childhood, and the patient had a destroyed lung due to bronchiectasis that developed with the compression of the main bronchus by the mediastinal mass. Although the CT images of 5 years ago were not available, a report for a bronchial compression or a destroyed lung were not mentioned at that time. Current thorax CT showed that, the mediastinal mass doubled in size and due to the bronchial compression the lung parenchyma was destroyed.Differential diagnosis is important in patients with mediastinal mass. For this reason, establishment of the diagnosis by preoperative PET/CT and a tissue biopsy is recommended [5]. Such as, a diagnosis of lymphoma obtained by biopsy will direct the primary treatment of the patients mostly medically. In our case, the mediastinal mass was suitable for a transbronchial biopsy and PET-CT could have been done. However, the patient with the destroyed lung had a definitive indication for a surgical intervention so the former interventions had not been performed. Left pneumonectomy and mediastinal mass excision were performed for definite diagnosis and treatment.
CLL patients may be asymptomatic at the time of diagnosis or present with B symptoms (weight loss, fever, night sweats), pallor caused by anemia, hemorrhage due to thrombocytopenia, symptoms due to lymph node or organ involvement, and frequent infections because of hypogammaglobulinemia. The most common finding on physical examination is lymphadenopathy (LAP), and splenomegaly. Hepatomegaly can also be seen [6]. Thoracic complications are not uncommon in hospitalized patients with CLL, but the specific etiology and incidence of these complications are limited [7]. Our case had nonspecific symptoms such as cough and chest pain at the time of admission. When the literature is reviewed, CLL cases with bronchial compression due to mass effect after mediastinal involvement and causing destroyed lung are rare [8].
In conclusion, the coexistence of CLL, which causes bronchiectasis and destroyed lung by compressing the bronchi with mass effect, is rare. Hematological malignancies should be kept in mind in the presence of bronchiectasis and mediastinal mass for which surgery is considered.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Authors’ contributions
CH, KCC; conceived and designed the current case report. FC; collected the clinical data, AGY; examined the pathological preparates. KCC, CH, FC; co-wrote the paper. All authors discussed the case with under the literature data and contributed to the final manuscript.
Reference
1) Conlan AA, Lukanich JM, Shutz J, Hurwitz SS. Elective pneumonectomy for benign lung disease: modern-day mortality and morbidity. J Thorac Cardiovasc Surg 1995; 110: 1118-24.
2) Yalçınkaya İ, Özbay B. Harap akciğer (iki olgu sunumu). Van Tıp Der 2001; 8: 79-81.
3) Halezeroglu S, Keleş M, Uysal A, Celik M, Senol C, Haciibramoğlu G et al. Factors affecting postoperative morbidity and mortality in destroyed lung. Ann Thorac Surg 1997; 64: 1635-8.
4) Mısırlıoğlu AK, Bayram S, Kıral H, Ağca MÇ, Akyıl FT, Alpay L et al. Factors affecting complication rates of pneumonectomy in destroyed lung. Turk Gogus Kalp Damar Cerrahisi Derg 2018; 26: 272-8.
5) Kim BT, Lee KS, Shim SS, Choi JY, Kwon OJ, Kim H et al. Stage T1 non–small cell lung cancer: preoperative mediastinal nodal staging with integrated FDG PET/CT - a prospective study. Radiology 2006; 241: 501-9.
6) Rai KR, Sawitsky A, Cronkite EP, Chanana AD, Levy RN, Pasternack BS. Clinical staging of chronic lymphocytic leukemia. Blood 1975; 46: 219-34.