



2Department of Thoracic Surgery, Sanliurfa Research and Training Hospital, Sanliurfa, Turkey DOI : 10.26663/ cts.2022.009
Summary
Although sternum fractures are more common after direct and impact trauma, they are rarely caused by pathological reasons. Sternum insufficiency fractures have been reported rarely in elderly patients. In the literature, sternum fracture after low-energy indirect trauma has been rarely reported. Our aim in this case is to present a 79-year-old female patient with chest pain after indirect trauma and a sternum fracture on admission to the emergency department. The patient with previously known Parkinson’s disease had a manubrium sternum fracture on computed tomography, and no additional pathology was found.Introduction
Insufficiency fractures are common in the spine, pelvis, and lower extremities [1]. Insufficiency fractures are rarely seen in the medial femoral condyle, talus, sternum, first rib, and sacrum [2]. Sternum insufficiency fractures are often seen in the body of the sternum and rarely in the manubrium [3]. Insufficiency fracture can be seen secondary to recurrent minor traumas, lymphoma, metastatic involvement, corticosteroid use, osteoporosis [3]. Sternum insufficiency fractures may be associated with dorsal kyphosis or without kyphosis, may be symptomatic or asymptomatic, and may be confused with pathological fractures [4].Parkinson’s disease is one of the most common neurodegenerative diseases [5]. The incidence of Parkinson’s disease is increasing due to reasons such as prolongation of life span and industrialization. It is predicted that the number of Parkinson’s patients will exceed 12 million worldwide by 2040 [6]. Postural instability is an important symptom of Parkinson’s disease and may be present at the time of diagnosis; resulting in an increased risk of falling, loss of independence, and impaired quality of life [7]. Postural control is impaired in more than 75% of Parkinson’s patients, so the postural instability and the risk of falling increases [8].
In this case, we aim to emphasize that sternum insufficiency fractures may develop due to thoracic vertebral kyphosis in Parkinson’s patients.
Case Presentation
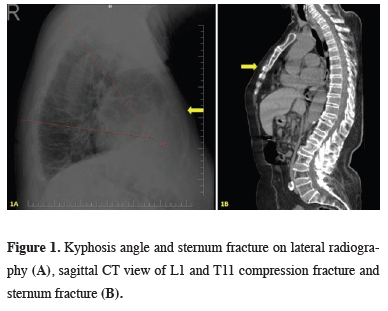
A 79-year-old female patient admitted to the emergency department in January 2021 due to anterior chest pain. It is known that the patient fell on the right shoulder at her height on the day of admission, and pain developed in the anterior rib cage after falling. She had no comorbid disease other than the known Parkinson’s disease and no history of previous trauma. There was no cardiac or pulmonary finding in her system query. She did not smoke or drink alcohol. She had tremors and localized chest pain on physical examination. No skin infection and emphysematous changes, ecchymosis, or crepitation on the chest wall were found. No fracture was observed in the right shoulder joint examination and imaging. Hemoglobin was 13.3 g/dL, Troponin T was 5.48, and CK-Mb was 1.39 (ref value < 4.88) on admission to the emergency department. No pathology was found on electrocardiography at the first admission. Cardiac and pulmonary pathologies were ruled out. A fracture in the manubrium sternum was detected in the lateral graphy (Figure 1a) and computed tomography (CT) of the patient (Figure 1b). Cobb angle and kyphotic angle (< 45°) were measured on lateral radiography (Figure 1a).){kind=link}
 Click Here to Zoom |
Figure 1: Kyphosis angle and sternum fracture on lateral radiography (A), sagittal CT view of L1 and T11 compression fracture and sternum fracture (B). |
Since the patient did not require surgical treatment, she was followed up in the thoracic surgery service for conservative treatment and follow-up. Bone mineral density (BMD) measurement was requested in terms of osteoporotic fracture exclusion due to the presence of kyphotic changes in T11 and L1 in the sagittal CT section (Figure 1b). The T-score in the left femur/total hip region was found to be -1.9 while the BMD value was found to be -1.7 in the lumbar region, and it was considered osteopenic. Blood D-vitamin level was 5.80, calcium was 9.05 mg/dL, alkaline phosphatase was 66 U/L and primary vitamin D deficiency was detected.
In the retrospective anamnesis of the patient, it was learned that the patient had Parkinson’s disease for 12 years and had been using pramipexole 1mg (parkipex, Generica İlaç San. ve Tic A.Ş.), domperidone 10 mg (Motilium, Johnson& Johnson), benserazide hydrochloride 125 mg (Deva Holding A.Ş.) and rasagiline 1 mg (Rasalas, Abdi Ibrahim). During the follow-up of the patient, when her tremors continued at the current drug doses, dose changes were made in consultation with the neurology and the tremors regressed. The patient was discharged with a daily dose of 1200 IU vitamin D and an appropriate analgesic treatment. She recovered without sequelae after 3 months in her follow-up. The case review was conducted according to all guidelines outlined in the Declaration of Helsinki. Written informed consent for publication was obtained from the patient and patient’s nearest relative.
Discussion
Musculoskeletal pathologies are common in patients with Parkinson’s. Age, female gender, disease severity and advanced age are predisposing factors for musculoskeletal pathologies [9]. Postural instability and tremor are major findings in Parkinson’s disease; besides, postural abnormalities, gait disorders, speech disorders, hypomimia, changes in eye movements are among other motor findings [9]. After postural instability, patients develop kyphosis to maintain balance. Osteopenia and osteoporosis is a common finding in Parkinson’s patients [10]. Compression fractures seen after extensive osteopenia in elderly patients also cause dorsal kyphosis. Our case had osteopenia, compression fracture, and dorsal kyphosis developed due to Parkinson’s disease. Kyphosis creates flexion-compression stress in the sternum, resulting in sternum insufficiency fractures. In elderly patients, the osteopenic structure of bones and loss of elasticity of cartilage tissue are predisposing to insufficiency fractures [4].In a review published in France in 2015, it was reported that falling alone was not a risk factor for fracture in Parkinson patients. Decrease in physical activities due to loss of neuromuscular function, malnutrition, low body mass index, high parathyroid hormone, low vitamin D level, and especially the use of antiparkinsonian drugs such as L-dopa cause weakening of bone quality and atraumatic fractures [9].
Sternum fractures are more common after high-energy traumas, but they are rare. Insufficiency fractures most commonly occur in lower extremities, vertebra and pelvic bones. Sternum insufficiency fractures are extremely rare, more common in elderly patients. It is often in the manubrium zone of the sternum [3]. Our case has a manubrium sternum insufficiency fracture.
The thorax is stabilized by the ribs, sternum, and vertebrae. Insufficiency of one of these structures creates additional stress to other structures. According to Fowlers’ flexion-extension compression theory: after multiple osteoporotic thoracic vertebra compression fractures, secondary sternum insufficiency fracture may develop against flexion and compression stresses caused by chronic thoracic kyphotic deformity [1,3]. In this case, the patient had no history of previous vertebral trauma, but she had thoracic kyphosis on T11 and L1 due to compression fractures. It is thought that the patient developed secondary insufficiency fracture due to thoracic kyphosis deformity.
Sternum insufficiency fractures are divided into two as buckling or non-buckling. Buckling fractures are associated with thoracic kyphosis, while non-buckling fractures may or may not be associated with thoracic kyphosis. Our case had a buckling type sternum insufficiency fracture. With lateral chest radiographs, the localization of the sternum fracture can be determined, as well as thoracic kyphosis. CT can be used to exclude infection and malignancy [1].
In conclusion, thoracic kyphosis and sternum insufficiency fractures are associated, they are not very common. Over this rare situation, it should be considered that sternum insufficiency fracture may occur in patients with thoracic kyphosis and osteopenia after urgent cardiac and pulmonary causes are ruled out in patients admitting with anterior chest pain. Insufficiency fractures cause significant morbidity and mortality in the elderly group. Future insufficiency fractures and complications can be prevented, hospital stay times and costs can be reduced with osteoporosis treatment.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Authors contributions
ÖO,FC; conceived and designed the current case report, co-wrote the paper, FC: collected the clinical data. The authors discussed the case under the literature data together and constituted the final manuscript.
Reference
1) Jun-Ki Min, Hyun-Jung Joo, Tae-Ho Kim, Jin-Hong Yoo, Mi-Sook Sung, Chul-Soo Cho et al. A Case of Sternal Insufficiency Fracture. Korean J Intern Med. 1999; 14: 94-7.
2) Vaishya R, Agarwal AK, Banka PK, Vijay V, Vaish A. Insufficiency Fractures at Unusual Sites: A Case Series. J Orthop Case Rep 2017; 7: 76-9.
3) Abrahamsen SØ, Madsen CF. Atraumatic sternum fracture. BMJ Case Rep 2014; 2014: bcr2014206683.
4) Sapherson DA, Mitchell SC. Atraumatic sternal fractures secondary to osteoporosis. Clin Radiol 1990; 42: 250-1.
5) Balestrino R , Schapira AHV. Parkinson disease. Eur J Neurol 2020; 27: 27-42.
6) Dorsey ER , Sherer T, Okun MS , Bloem BR. The Emerging Evidence of the Parkinson Pandemic. J Parkinsons Dis 2018; 8: S3-S8.
7) Kim SD, Allen NE, Canning CG, Fung VS. Postural instability in patients with Parkinson’s disease. Epidemiology, pathophysiology and management CNS Drugs 2013; 27: 97-112.
8) Gandolfi M, Geroin C, Dimitrova E, Boldrini P, Waldner A, Bonadiman S et al. Virtual Reality Telerehabilitation for Postural Instability in Parkinson’s Disease: A Multicenter, Single-Blind, Randomized, Controlled Trial. Biomed Res Int 2017; 2017:7962826. doi: 10.1155/2017/7962826.