



Summary
Nail gun injuries have been reported in the medical literature since the introduction of these tools in 1959. The number of injury cases is increasing over time due to the increasing use of nail guns in the construction industry. While the most common site of nail gun injuries is non-dominant hand and fingers, rarely head, thoracic, abdominal, and cardiac injuries have been reported. Depending on the injured organ, the primary method of treatment for such injuries, which have catastrophic consequences, is appropriate surgical interventions.Introduction
Since their introduction in 1959, nail guns are increasingly used in the modern construction industry due to being inexpensive, easy-to-access, and time-saving tools [1]. In general, it is estimated that the mortality rate of nail gun injuries is similar to stabbing injuries. Injuries mostly occur in limbs such as hands and feet. Abdominal, cranial, thoracic, and cardiac injuries are much less common. The primary method of treatment is surgery [2,3].Here, we present a patient with a rare transsternal injury and suspicion of tracheal perforation who was preferred to be treated conservatively, and his treatment strategy for discussion.
Case Presentation
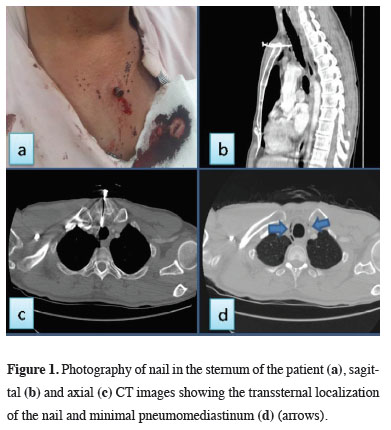
A 37-year-old male patient, a furniture worker, was admitted to a local hospital in July 2020 for injury to the chest area by a nail bounced after the firing of a nail gun. The patient who had stable vital signs and no active bleeding on initial examination was referred to our hospital for further treatment and intervention after the administration of tetanus prophylaxis. The examination of the patient with no active bleeding revealed a nail in the sternum above the manubrium sterni about 2 cm below the incisura jugularis (Figure 1a).){kind=link}
 Click Here to Zoom |
Figure 1: Photography of nail in the sternum of the patient (a), sagittal (b) and axial (c) CT images showing the transsternal localization of the nail and minimal pneumomediastinum (d) (arrows). |
The respiratory sounds of the patient with a blood pressure of 110/70mmHg, a heart rate of 72/min, and a respiratory rate of 15/min, who did not describe hemoptysis, were auscultated normal. The laboratory tests showed that Hb was 15mg/dL, and WBC was 12,000/mm3. The patient with a stable condition underwent contrast-enhanced computed tomography of the chest (CT) and neck to determine the relationship of the injury with the great vessels and the trachea. His CT showed a foreign body extending from the sternum to the anterior wall of the trachea, and pneumomediastinum (Figures 1b-d).
The foreign body was found to have a distance from the major vessels, but the possibility of tracheal injury could not be excluded. After the patient was transferred to the operating room and all equipment, including sternotomy, was prepared, bronchoscopy was first performed under general anesthesia and the trachea was checked. In the operating room, the patient’s trachea was observed to be intact, and the nail was removed by pulling backward manually in accordance with the tract line. The patient with no active bleeding and no air leak was kept under general anesthesia in the operating room for 20 minutes. The patient, who had no change in vital signs and no bleeding, was transferred to the intensive care unit and closely monitored. For prophylaxis, he was given 2 grams of ampicillin 3 times a day. Daily acute phase reactants and close hemoglobin monitoring were performed. No increase was detected in CRP, procalcitonin values and WBC count. Also no decrease was identified in Hgb value. The oral intake of the patient, who was followed up without oral intake for two days, was initiated gradually since he had no swallowing difficulty or respiratory complaints. He did not have fever during the follow-ups. On day 5 of the follow-up, the patient was discharged with recommendations. Written informed consent was obtained from the parents for publication of his data.
Discussion
Nail gun injuries have been reported in the medical literature since their introduction in 1959 [1]. Basically, nail guns are produced in 2 different forms as slow-speed nail guns triggered by a pneumatic system and high-speed nail guns triggered by an explosive cartridge. While the velocity of the fired nails ranges from 97.7 to 121.1 ft/s in such tools, this velocity can reach up to 300-2200 m/s in conventional weapons [4].These tools are used in the construction industry on wood, plastic, light metal, and even concrete surfaces. Although special permits are required for high-speed tools, slow-speed ones can easily be supplied in daily life without training. The incidence of such injuries increases with the increasing use of nail guns in the construction industry. Nail gun injuries mostly occur in adults in the form of occupational accidents. There are also rare reported cases of suicide and children [2,3].
The most common site of injury is hand and fingers, followed by wrist, forearm, foot and toes, knee, and eye. Abdominal, thoracic, cranial, and cardiac injuries are much less common. The mortality rate varies depending on the velocity, size of the nail, and the injured organ. Although overall mortality rates are similar to stabbing injuries (25%), unlike firearm and stabbing injuries, sudden abundant bleeding is rare, including cardiac injuries [5].
This is due to the fact that the object (nail) causing the injury still remains in the tissue. Therefore, it should be kept in mind that abundant bleeding may occur when the foreign body is removed [6].
General recommendations for keeping such patients alive are rapid interventions. Unstable patients should be immediately transferred to the operating room without any examination. Thoracic injuries are mostly seen on the anterior thoracic wall. Therefore, anterior thoracotomies are primarily preferred depending on the location of the injury. Median sternotomy is preferred for precordial injuries. In stable patients, hemothorax, pneumothorax, pneumomediastinum, and other complications can be preoperatively evaluated using imaging techniques such as chest radiographs, and thoracic CT. In the literature, conservative treatment is a treatment modality mostly preferred for limb injuries [2,3].
Our patient underwent thoracic CT to evaluate the trachea more clearly, because of being hemodynamically stable and the location of the injury. The CT showed pneumomediastinum and the close relationship of the sharp tip of the foreign body with the trachea. However, tracheal injury could not be excluded. Although the patient did not complain of hemoptysis, it was thought that any bleeding that may result from the removal of the foreign body may jeopardize the patient by filling the trachea from an injury to the trachea. After all preparations were made for a possible sternotomy in order to reduce potential risky situations, it was decided to determine the condition of the trachea clearly by performing bronchoscopy under general anesthesia in the operating room setting. In the case of an injury, it was planned to protect the patient’s airway from possible bleeding by pushing the endotracheal tube cuff distally to the injury to secure the airway. Therefore, fiberoptic bronchoscopy was primarily performed under general anesthesia, although it has never been used for such patients. After ensuring that the trachea was intact, the nail in the sternum of the patient was removed manually while the patient was intubated. After waiting for 20 minutes in the operating room for any active bleeding following the removal of the nail, the patient was transferred to the intensive care unit.
Nail guns are tools with the potential to cause catastrophic bleeding and fatal injuries. Basically, prevention and education are the most appropriate ways to reduce mortality caused by these injuries. In thoracic injuries, it should be kept in mind that conservative treatment can be used for patients with a stable condition, no active bleeding, and confirmed to have no organ injury, even in cases of transsternal injuries, provided that all measures are taken for emergency intervention in, while unstable patients should be rapidly intervened.
It is seen in the literature that the frequency of injuries related to nail guns has increased due to the rapid developments in the construction sector. We are in favor of modifying such devices in order to prevent this situation and to reduce the possibility of injury. Nail guns can be fired very easily. There are types that can be fired even without coming into contact with a rigid structure. From our point of view, these guns should not be able to be fired without touching a hard surface. At the same time, we believe that it will seriously reduce possible accidents that may occur a few seconds between ignitions after being triggered. Another important point is that the firing speed of pneumatic nail guns is higher than many guns. Therefore, these types of nail gun uses must be subject to special permissions.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Authors’ contributions
OFD,OO,OT: conceived and designed the current case report, co-wrote the paper, collected the clinical data. The authors discussed the case under the literature data together and constituted the final manuscript.
Reference
1) Cragg J. Nail-gun fatality. BMJ 1967; 4: 784.
2) Wang SH, Chen MY, Yan JL, Huang TY, Chang CC, Chien CY. Survival after multiple nail gun injuries to brain, lung, and heart: a case report and review of the literature. J Int Med Res 2021; 49: 03000605211049923.
3) Kulaylat AN, Chesnut III CH, Patel S, Rocourt D, Clark JB. Penetrating cardiac nail gun injury in a child. Pediatr Emerg Care 2016: 32: 536-7.
4) Tuladhar S, Eltayeb A, Lakshmanan S, Yiu P. Delayed presentation of right and left ventricle perforation due to suicidal nail gun injury. Ann Cardiac Anaesth 2009; 12: 136-9.