



Summary
Pulmonary sequestration is a congenital anomaly which receives its blood supply from systemic circulation It has no connection with normal tracheobronchial system, and located in a pulmonary lobe. These lesions should be treated promptly by surgery. Minimally invasive techniques may be preferred for resection. In the 32-year-old female patient, a lobulated, well-circumscribed mass lesion with a diameter of approximately 4 cm was detected on the posterior basilar segment of the left lower lobe. Besides, an aberrant artery which originated from the thoracic aorta and feeding the lesion was found. It was preoperatively observed that the arterial supply of the lesion was approximately 2 cm in diameter, originating from thoracic descending aorta. Venous drainage was through the pulmonary vein. Since intraoperative findings proved intrapulmonary sequestration to be necessary, left lower lobectomy was performed by VATS. The final pathology result was also reported as intralobar sequestration. This case is presented due to its rare occurrence and the use of minimally invasive techniques.Introduction
Pulmonary sequestration is a congenital anomaly which located in a pulmonary lobe [1]. While it receives its blood supply from the systemic circulation, the venous drainage may be through pulmonary system, azygos vein or portal system. The incidence ranges from 0.15% to 6.4% [2]. Two types are defined as, intralobar pulmonary sequestration (25%) and extralobar pulmonary sequestration (75%). They may remain asymptomatic, but some complications such as intrapulmonary hematoma, hemothorax and aspergilloma may also develop or there may be a malignant transformation to carcinoid tumor, adenocarcinoma, squamous cell carcinoma, sarcoma, or pulmonary blastoma. Therefore, these lesions should be surgically treated promptly. In order to emphasize the importance of surgical treatment, we wanted to present a case of left lower lobectomy by VATS due to intrapulmonary sequestration.Case Presentation
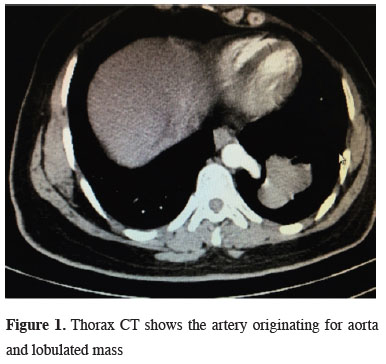
32-year-old female patient applied to chest diseases outpatient clinic for a routine check-up before starting up a new job. In the chest radiography, a hyperdense lesion was seen in the left lower zone. In the contrast enhanced thoracic computed tomography, in addition to a lobulated, well-circumscribed mass with a diameter of approximately 4 cm in the posterior basilar segment of the left lower lobe, a large arterial supply, which was approximately 2 cm in diameter originating from the thoracic aorta was detected (Figure 1). Venous drainage was through the pulmonary vein.){kind=link}
 Click Here to Zoom |
Figure 1: Thorax CT shows the artery originating for aorta and lobulated mass |
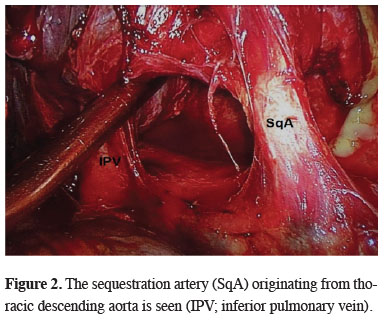
On physical examination, no pathology was detected. The patient was hospitalized with the pre-diagnosis of intrapulmonary sequestration. Fiber-optic bronchoscopy was performed to display the bronchial tree in the preoperative period. Neither any endobronchial lesion nor abnormal bronchial connection that may be associated with the lesion in the left lower lobe was found. A utility incision of 3.5 cm was made through the 6th intercostal space and a 1.5 cm thoracoport incision was placed at the 8th intercostal space and videothoracoscope was placed in the left hemithorax. Adhesions between the left lower lobe and diaphragm were carefully separated. Pulmonary ligament was dissected carefully. The sequestration artery originating from thoracic descending aorta was revealed (Figure 2) and divided with endoscopic vascular stapler. Then the lower lobectomy was completed and did not encounter any complications. A chest drain was placed in the thoracic cavity. The patient did not have any problems during postoperative period and was discharged on the 3rd day following the operation. The pathological result was reported as intralobar sequestration. The patient is still under outpatient clinic follow-up.
){kind=link}
 Click Here to Zoom |
Figure 2: The sequestration artery (SqA) originating from thoracic descending aorta is seen (IPV; inferior pulmonary vein). |
Discussion
Intralobar pulmonary sequestration is a rare congenital anomaly. It can be detected as an incidental pulmonary lesion. The patients may be asymptomatic as in our patient. However, more commonly, they may present variable pulmonary symptoms such as pleural effusion or recurrent pneumonia, and sometimes with aspergillosis and fatal hemoptysis. Therefore, sequestration is usually treated by resection of the affected area of the lung [3].In intralobar sequestration, abnormality is seen as an intrapulmonary lesion in the posterobasal segment of the left lower lobe as displayed in our case. The right lower lobe can be affected in about one third of the cases [2]. Although reports of conservative treatments of pulmonary sequestration, such as spontaneous involution and arterial embolization, have been published, the treatment is commonly surgery even in asymptomatic patients. Before the surgery, antibiotic treatment and respiratory physiotherapy should be performed and if any, infection should be kept under control.
It is proved that VATS is a safe and feasible surgical procedure in experienced hands [4]. The difficulty of resection is to identify the abnormal artery. In the region of sequestration due to frequent recurrent infections, there are usually inflammatory changes and the artery is hidden under the inflamed tissue. There may be very dense adhesions and inflamed tissue may mimic the artery. Abnormal arteries or veins should be identified carefully at the beginning of the procedure [5]. There were adhesions between the lower lobe and diaphragm in our case as well; however, due to the recognition of the intrapulmonary sequestration in preoperative period and display of the abnormal systemic artery, the systemic artery was dissected carefully and divided properly.
As a conclusion, the treatment of pulmonary sequestration is surgery. In such cases, VATS can be safely performed in experienced hands. It is important to perform dissection carefully and to display the abnormal artery. Resection by VATS reduces morbidity and shortens duration of stay in the hospital.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Reference
1) Çubuk S, Çaylak H, Gözübüyük A, Yücel O, Gürkök S. Literatürde bir ilk: Persistan sol superior vena kava ile intralober sekestrasyon birlikteliği. Gulhane Tıp Derg 2015; 57: 294-6.
2) Abbey P, Das CJ, Pangtey GS, Seith A, Dutta R, Kumar A. Imaging in bronchopulmonary sequestration. J Med Imaging Radiat Oncol 2009; 53: 22-31.
3) Hertzenberg C, Daon E, Kramer J. Intralobar pulmonary sequestration in adults: three case reports. J Thorac Dis 2012; 4: 516-519.