



Summary
In this case report, the case of non-small cell lung cancer resection performed with surgeon-powered robotic surgery (sPRS) was evaluated in light of the literature. A 62-year-old male patient applied to our clinic with the complaint of non-specific chest pain. On the tomography of the patient, a mass of approximately 1 cm in the lower lobe of the right lung was detected, and there was no distant metastasis. A transthoracic needle biopsy was performed on the patient. Right lower lobectomy operation was performed using wristed instruments (Artisential® Wristed Instruments) in this non-small cell lung cancer patient. sPRS provides more mobility than VATS and we think that it is a more cost effective surgical instrument than robotic surgery. We think that surgeons should embrace new technologies in order to provide more benefits to patients.Introduction
With developing technologies, lung cancer surgeries have been changing from video thoracoscopic surgery (VATS) to robotic-assisted thoracic surgery (RATS). Robotic surgery has developed due to the lack of flexibility and maneuverability in VATS [1]. However, it is still not widely preferred today in terms of cost and effectiveness. For this reason, different technologies have been developed in which VATS has been combined with robotic technology.Nowadays, the results of robotic surgeries and VATS operations are frequently compared. However, publications have stated that robotic surgical procedures have been more successful than VATS in the early postoperative results [2-4]. On the other hand, one of the main limitations in VATS surgery is limited freedom, since the surgical instruments do not have sufficient angles during the surgery. Wristed VATS instruments are a new technology introduced as an alternative to robotic surgery. Trevis et al. [2] were the first in the literature to define the technology of these instruments as surgeon-powered robotic surgery (sPRS). Today, it is becoming increasingly popular due to the possibility of movement with sPRS technology that is the same as with RATS technology. However, only two studies in the literature used these instruments in thoracic surgery operations [2,3].
In this case report, a case of non-small cell lung cancer resection performed with sPRS technology was evaluated with the literature.
Case Presentation
A 62-year-old male patient applied to our clinic with the complaint of non-specific chest pain. A mass of approximately 1 cm was detected in the lower lobe of the right lung on the tomography of the patient, who had a history of smoking 30 packs of cigarettes/year and also had diabetes mellitus. Surgery was planned for the patient, who did not have distant metastases on positron emission computed tomography (PET-CT) and was found to have non-small cell lung cancer via transthoracic fine-needle aspiration biopsy. In the patient, who was operated on with sPRS, a thoracoport was opened for an instrument of 2 cm from the 4th mid-axillary intercostal space and the 7th posterior axillary line. A 3-cm utility incision was made in the subcostal space. Thoracic pathologies, adhesions, and the diaphragm level were evaluated using a 30° 10-mm thoracoscope (Logic HD, Storz, Germany) using a subcostal incision. During the exploration, a mass was detected in the lower lobe of the right lung. Articulated thoracoscopic precise dissector (38-cm shaft, Artisential) were used for dissection of the pulmonary veins and arteries. A precise dissector wristed instrument was used from the 4th midaxillary incision. Articulated thoracoscopic forcep (38-cm shaft, Artisential) were used for traction of the lung. A forcep wristed instrument was used from 7th posterior axillary incision. Pleural adhesions were severed using robotic arm bipolar cautery. The pulmonary arteries, veins, and bronchus were ligated with endoscopic closure devices (endoGIA, Covidien plc, Norwalk, USA). Right lower lobectomy operation was performed on the patient using wristed instruments (Artisential Wristed Instruments) (Figures 1,2). Specimens were removed using endoscopic specimen bags. Systematic lymph node resection was done from stations 2, 4, 7, 8, 9, and 11. The patient, whose postoperative pathology was reported as squamous cell carcinoma, was discharged three days postoperatively. Informed consent was obtained from the patient.){kind=link}
){kind=link}
 Click Here to Zoom |
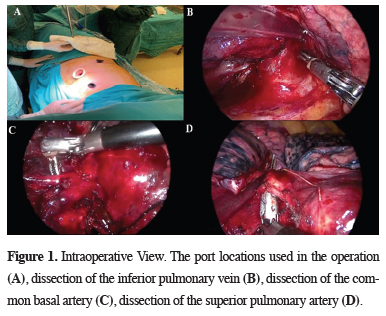
Figure 1: Intraoperative View. The port locations used in the operation (A), dissection of the inferior pulmonary vein (B), dissection of the common basal artery (C), dissection of the superior pulmonary artery (D). |
 Click Here to Zoom |
Figure 2: Intraoperative view; use of the instruments. |
Discussion
Video thoracoscopic surgeries have become increasingly common nowadays. The rigidity of the instruments sometimes makes it difficult to perform operations. On the other hand, wristed laparoscopic instruments have begun to be used as an alternative today, in terms of both cost-effectiveness and safety.Especially in publications that have been made with regard to robotic surgery, it has been stated that it is oncologically similar to VATS. However, the operation time is very long due to docking. In their series of 103 cases, Novellis et al [4] found that the length of stay in RATS was more successful when compared to open surgery and VATS. Oncologically, they stated that lymph node dissection could be performed as much as open surgery. In addition, it was stated in the literature that pain in RATS is less than in other techniques. Similarly, Alhan et al [5] stated that the pain was less in the operations performed with RATS. Trevis et al [2] reported on a case series in the literature on sPRS and stated that when compared to RATS, it had similar motion advantages and was more advantageous in terms of cost-effectiveness. In addition, Fianan et al [6] stated in their study that technical problems in robotic technologies were observed at a rate of 8.2%. They mentioned that these technical problems would be improved with future technological developments. In sPRS technology, on the other hand, it is believed that these technical problems have been eliminated due to the absence of a computer systems.
In the current case, the most important reason for preferring these instruments for surgical resection is the possibility of 360° movement. Since one of the most important problems in VATS surgery is the limitation of movement, it is believed that resections will be easier with these instruments. In addition, it is believed that it provides an advantage in the dissection of vascular structures, because it has a tactile impulse that is similar to VATS. With these instruments, it is believed that the minimally invasive technique will evolve into a microinvasive technique in the coming years.
In the current case, subcostal incision was preferred over utility incision, which is used in VATS. During the tumor removal, the specimen could be removed from the subcostal area more easily than the intercostal area, which is much more rigid than the subcostal area. Especially in recent years, subcostal approaches have been more preferred in thoracic surgery because they are less painful [7]. On the other hand, this case was the first case performed in Turkey using sPRS technology.
One of the disadvantages of robotic surgery is that it does not have a tactile impulse in the most important surgeries. The absence of palpation or tissue sensation of the tumor may create additional difficulty in the operation. Robotic operations require experience in a certain number of simulations [8]. Since sPRS has a similar structure to VATS, it is believed that the learning period of the instruments is much faster.
The fact that the surgeon is positioned at the operating table during the operation is among the advantages of VATS and sPRS. In addition, CO2 insufflation after the operation also prevents enlargement of the incision.
In conclusion, sPRS provides more mobility than VATS and it is believed that it is a more cost-effective surgical instrument than RATS. It is believed that there will be serious changes in thoracic surgery in the following decades, and that the developments in robotic surgery and minimally invasive approaches will allow surgeons to more easily perform microscopic operations in the future. It is believed that surgeons should embrace new technologies in order to provide more benefits to patients.
Declaration of conflicting interests
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
Funding
The authors received no financial support.
Authors’ contributions
CBS, MM: conceived and designed the current case report, co-wrote the paper, CBS: collected the clinical data. The authors discussed the case under the literature data together and constituted the final manuscript.
Reference
1) Cosgun T, Kaba E, Ayalp K, Alomari MR, Toker A. Robot-Assisted Thoracoscopic Surgery: Pros and Cons. Curr Surg Reports 2017; 5: 1-6.
2) Trevis J, Chilvers N, Freystaetter K, Dunning J. Surgeon-powered robotics in thoracic surgery; an era of surgical innovation and its benefits for the patient and beyond. Front Surg 2020. https://doi.org/10.3389/fsurg.2020.589565
3) Cho S. Video-Assisted Thoracic Surgery Thymectomy: Subxiphoid Approach. J Chest Surg 2021; 54:314-8.
4) Novellis P, Bottoni E, Voulaz E, Cariboni U, Testori A, Bertolaccini L et al. Robotic surgery, video-assisted thoracic surgery, and open surgery for early stage lung cancer: Comparison of costs and outcomes at a single institute. J Thorac Dis 2018; 10: 790-8.
5) Alhan C. Robot-assisted mitral valve surgery without aortic cross-clamping: An alternative technique. Turk Gogus Kalp Damar Cerrahisi Derg 2021; 29: 415-6.
6) Finan MA, Rocconi RP. Overcoming technical challenges with robotic surgery in gynecologic oncology. Surg Endosc 2010; 24: 1256–60.